Protocols
Protocol 100: Medication Administration
1. FIRST, DO NO HARM: Medication errors are the most common AVOIDABLE error that causes patients direct harm. When in doubt, contact ON DUTY MEDICAL CONTROL for any questions concerning dosage.
2. VERIFY “5 RIGHTS”:
- right patient
- right drug
- right dose
- right route (IV, IO, IM, SC, etc)
- right time (including rate of administration)
3. DOCUMENTATION: document accurately all medications administered, any reaction to medication, repeat vital signs after administration, and any adverse events.
4. MEDICATION ERRORS: Any error in medication administration should be documented and reported immediately through the CQI process to the Medical Director / Liaison for review. The goal of CQI review is to determine and minimize systemic contributions to causality of errors, not to take punitive action.
5. PEDIATRICS: Errors in pediatric medication dosing occur more often due to poor estimates of weight or infrequent use of pediatric doses. Every effort must be made to obtain accurate weight estimates, accurate calculation of dose, and appropriate monitoring of patient response. When in doubt, contact MEDICAL CONTROL for verification of dosage. Standardized tools to determine dosing in critical situations, such as a ‘pedi-wheel’ or Broslow tape, are encouraged.
*****When calculating pediatric doses, NEVER ROUND UP*****
Protocol 101: IV Fluid Administration
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Isotonic crystalloids provide volume replacement to maintain blood pressure and perfusion. The mechanism in trauma is far more complex, as aggressive fluid replacement often worsens blood loss and hypothermia.
INDICATIONS: dehydration, syncope, sepsis, medication administration, right-sided myocardial infarction, undifferentiated cardiac arrest
CONTRAINDICATIONS: While small amounts of fluid may be used, large volume fluid administration should be avoided in acute CHF, major trauma, or dialysis patients. Hyperkalemia is a relative contraindication for Lactated Ringers (LR), as there is a small amount of potassium in LR. If there are signs of hyperkalemia on EKG, LR should not be used.
PRINCIPLES OF ADMINISTRATION:
1. LR is the preferred volume replacement fluid for most situations. This is especially true for trauma and sepsis.
2. Normal Saline, 0.9% NaCl, should be limited to use for mixing and administration of medications.
3. In major trauma, limit fluid resuscitation to those indications noted in trauma protocols.
4. Doses of fluids are specific to the medical/trauma indication, and the specific protocol should be referenced for amounts of fluid administration.
5. D10% use is addressed specifically under dextrose protocol and hypoglycemia.
6. D5%W may be utilized and transported by both AEMT and Paramedics under this protocol.
7. This protocol applies to all 911 and Interfacility Transfers for both AEMT and Paramedics.
CONSIDERATIONS:
- If supply chain limitations prohibit the use of LR, normal saline may be substituted until such time that LR is available.
- This protocol is specific to 911 calls, as interfacility transports may require patient-specific orders from the sending provider.
Protocol 102: Adenosine (Adenocard)
SCOPE: Paramedic ONLY
MECHANISM OF ACTION: temporary blockage of electrical conduction through the AV node in order to stop reentrant tachycardias involving the AV node (AVNRT, PSVT).
ONSET: 1 second
DURATION: 10 seconds
INDICATIONS: NARROW-complex supraventricular tachyarrhythmia CONFIRMED on 12 LEAD EKG
CONTRAINDICATIONS: Irregular tachyarrhythmia (Atrial fibrillation with RVR), wide-complex tachycardia, heart transplant, heart blocks
ADVERSE REACTIONS: chest pain, dyspnea (asthmatics), diaphoresis, palpitations, syncope
DRUG-DRUG INTERACTIONS:
- large amounts of caffeine hinder effect of adenosine, contact MEDICAL CONTROL for higher dose
- Dipyridamole (Persantine) enhances effect of adenosine, requiring REDUCED DOSE (typically 6mg). This medication is a platelet inhibitor, commonly prescribed to people who have artificial HEART VALVE replacement surgery.
- Carbamazepine (Tegretol) enhances effect of adenosine, prolonging AV node blockage. Consider REDUCED DOSE (typically 6mg)
DOSAGE:
ADULT: -12 mg IV bolus **RAPID** IV PUSH WITH RAPID 10 cc SALINE FLUSH
- Repeat dose of 12 mg if no conversion
- Contact MEDICAL CONTROL for further direction after second dose
PEDIATRIC: MEDICAL CONTROL APPROVAL is required for pediatric administration.
- Most children with SVT / AVNRT who are stable remain so and should be transported without medication / intervention.
- DOSE is 0.1mg/kg (max 6 mg initial dose), same **RAPID** administration as adults
- Repeat dose is 0.2mg/kg (max 12 mg)
CONSIDERATIONS:
- 12 LEAD should be printed before and after administration, with minimum of continuous 3 Lead documenting time of administration and response
- transient asystole or AV block should be expected right after administration
- for patients with unusual or atypical cardiac history (eg history of ablation, heart transplant) consider contacting MEDICAL CONTROL early for guidance and recommendations
Protocol 103: Albuterol Sulfate
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: Selective Beta-2 adrenergic agonist, resulting in potent bronchodilation of bronchi and alveoli.
ONSET: 5 – 10 minutes after inhalation
DURATION: 3-4 hours, though positive effects may decrease within the first hour, requiring additional doses
INDICATIONS: acute bronchospasm (may be intrinsic asthma or allergic etiology)
CONTRAINDICATIONS: Age > 60 with Severe tachycardia (>200), or concern for Acute MI
ADVERSE REACTIONS: tachycardia, palpitations, dysrhythmias (rare), hypokalemia, chest pain, may lower seizure threshhold
DRUG-DRUG INTERACTIONS:
- Beta-Blockers may decrease effectiveness of albuterol
- Sympathomimetics (eg pseudophedrine) may exacerbate adverse reactions
DOSAGE:
ADULT: OPTION 1 prescribed Metered Dose Inhaler
- Assist patient with inhalation of two 90mcg/spray (two ‘puffs’) every 10-15 minutes to a maximum of 6 puffs in 30 minutes
OPTION 2 Nebulized 2.5mg / 3ml saline
- Administer by nebulizer mask with minimum oxygen flow rate of 8 lpm.
- 3 total doses
- In severe asthma, all 3 doses may be used together as a continuous nebulizer
- Waveform capnography should be monitored for effect with continuous nebs
PEDIATRIC: (age > 1 year, or weight > 10 kg)
OPTION 1 prescribed Metered Dose Inhaler
- Assist patient with inhalation of two 90mcg/spray (two ‘puffs’) every 15-20 minutes to a maximum of 6 puffs in 45 minutes
OPTION 2 Nebulized 2.5mg / 3ml saline
- Administer by nebulizer mask with minimum oxygen flow rate of 8 lpm.
- 3 total doses
- Continuous nebulizer requires MEDICAL CONTROL approval
CONSIDERATIONS:
- Whenever possible, waveform capnography should be utilized to monitor degree of bronchospasm, CO2 retention and response to medication.
- EMT-Advanced and above should strongly consider concomitant use of Atrovent (Ipratropium) with initial nebulizer when indicated
- If patient presents with concern for hyperkalemia, contact MEDICAL CONTROL for authorization to use albuterol in these instances
- Albuterol is not the first line agent for anaphylactoid respiratory distress. Refer to epinephrine protocol first.
In line nebulizers may be used by EMT-Paramedics for field-intubated patients, with waveform capnography.
Protocol 104: Amiodarone
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Increases the refractory period of cardiac myocytes, prolongs Phase 3 repolarization by blocking potassium channels, decreases automaticity of ventricular and Purkinje fibers, prolongs AV conduction.
ONSET: 2-3 Minutes
DURATION: 1 to 3 hours (variable absorption and elimination makes this highly variable)
INDICATION:
AEMT: Pulseless arrest with shock-refractory or recurrent VT/VF
Paramedic Only: stable (not hypotensive), regular wide complex tachycardia
Paramedic Only: Narrow complex tachycardia, refractory to Adenosine
CONTRAINDICATIONS: A-V Heart blocks, cardiogenic shock, irregular wide complex tachycardia (obtain 12 Lead and contact MEDICAL CONTROL for consideration)
- do not use to treat PVCs, couplets or IVR rhythms
ADVERSE REACTIONS: hypotension, bradycardia
DRUG-DRUG INTERACTIONS:
- beta-blockers and calcium channel blockers may produce bradycardias or AV blocks,
- quinidine and propafenone (Rhythmol) may cause Torsades de pointes
DOSAGE:
ADULT:
AEMT: Pulseless VT / VF: 300mg IV bolus
- May administer ONE Additional 150mg IV bolus in 3-5 minutes if shock refractory or recurrent VF/VT
Paramedic Only: Stable (not hypotensive), regular wide complex tachycardia
- Obtain 12 lead first
- Contact MEDICAL CONTROL, if approved: 150mg IV bolus infusion over 10 minutes in 50 ml D5W/NS
Paramedic Only: Irregular wide complex tachycardia, Narrow complex tachycardia refractory to Adenosine, or Atrial Fibrillation with RVR
- Obtain 12 lead first
- Contact MEDICAL CONTROL, if approved: 150mg IV bolus infusion over 10 minutes in 50 ml D5W/NS
PEDIATRIC:
AEMT: Pulseless VT / VF:
- 5mg/kg IV bolus
- Additional doses require MEDICAL CONTROL approval
CONSIDERATIONS: Obtain 12 lead before and after administration in non-arrest patients.
Protocol 105: Aspirin
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: Inhibits platelet aggregation by blocking formation of thromboxane A-2
ONSET: Approximately 20 minutes
DURATION: Up to 96 hours
INDICATION: suspected Acute Myocardial Infarction or chest pain
CONTRAINDICATIONS: ACTIVE GI Bleeds, blood clot disorder, known aspirin sensitivity, pregnancy, children under age 2
ADVERSE REACTIONS: nausea, vomiting, heartburn, stomach pain, allergic reactions, tinnitus, bronchospasm
DRUG-DRUG INTERACTIONS: Interactions with other blood thinners SHOULD NOT interfere with the administration of Aspirin in a suspected Acute Coronary Syndrome
DOSAGE: 324mg PO, usually given as four 81mg chewable tablets
CONSIDERATIONS:
- Unless the patient has an active GI bleed or known sensitivity to aspirin, give to all suspected myocardial infarctions without delay.
- If patient has already taken 81mg ‘baby’ aspirin, personnel may administer the remaining 243mg
- If patient is uncertain if they have taken any aspirin in the past 24 hours, give the full 324mg
For young children age 2 to 12, chest pain is rarely caused by a myocardial infarction. Consider contacting MEDICAL CONTROL before administering to young children for chest pain.
Protocol 106: Atropine Sulfate
SCOPE: Paramedic ONLY
MECHANISM OF ACTION: Parasympatholytic blockage of vagus nerve tone to SA and AV nodes, resulting in increase heart rate. As the Vagus nerve normally inhibits the heart rate from going too fast, removing this inhibition may increase heart rate SO LONG AS the SA-AV-Purkinje system is functioning normally (i.e. there are no AV blocks). A secondary mechanism is seen with organophosphate poisoning, where atropine binds to acetylcholine receptors to decrease the effects of the excess acetylcholine caused by the poison.
ONSET: 1 minute
DURATION: 30-60 minutes (may last up to 3 hours in elderly patients)
INDICATION: Symptomatic bradycardia, heart blocks, organophosphate poisoning,
*** Epinephrine is First-Line medication for pediatric symptomatic bradycardia, Atropine is Second-Line.
CONTRAINDICATIONS: STABLE bradycardia
Atropine is NO LONGER INDICATED in PALS for pediatric cardiac arrest: See Epinephrine Protocol.
ADVERSE REACTIONS: agitation, confusion, blurred vision, pupil dilation, tachycardia, flushed skin, arrhythmias, dry mouth, worsening myocardial infarction
DRUG-DRUG INTERACTIONS:
- sympathomimetics may potentiate tachycardia
- in emergent situations, there are no acute interactions that would alter the decision to administer atropine
DOSAGE:
ADULT BRADYCARDIA: 0.5mg IV/IO bolus.
- Repeat at 3–5-minute intervals to a maximum dose of 3mg, or until effective to achieve improved cardiac output (improved blood pressure and mentation)
PEDIATRIC BRADYCARDIA: SECOND LINE MEDICATION, after use of EPINEPHRINE
- 0.02mg/kg (minimum 0.1mg) IV/IO bolus.
- Maximum single dose of 0.5mg.
- May give up to 1mg in adolescent if weight > 50kg.
- Contact MEDICAL CONTROL for repeat doses.
ORGANOPHOSPHATE POISONING: CONTACT MEDICAL CONTROL for orders. For adults, dosing regimen usually requires repeat doses of 2mg IV/IM every 10-15 min for moderate-to-severe toxicity that demonstrates respiratory compromise.
CONSIDERATIONS:
- Atropine should NOT be first-line medication in pediatric situations, consider epinephrine first.
- Dosing regimens to effectively treat organophosphate poisoning are often greater than the amount carried on an ambulance. Ensure effective decontamination of any substance on the patient by the appropriate hazmat-trained personnel before transport, then ensure rapid transport and early MEDICAL CONTROL notification.
Protocol 107: Atrovent (Ipratropium Bromide)
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: Parasympatholytic blockage of vagus nerve tone to mainstem bronchi and bronchiolar airways. When overstimulated by allergic or asthmatic reaction, vagal tone will result in cholinergic ‘flooding’ or excess acetylcholine production, which results in excess bronchiolar secretions, swelling and constriction. By blocking the vagal tone to the lungs, Atrovent limits further ‘flooding’ of the airways. It does NOT actively dilate the bronchi or alveoli, and therefore is only a ‘helper’ drug that should always be used in conjunction with Albuterol.
ONSET: 5 to 15 minutes.
DURATION: 6 to 8 hours (and therefore should only be given once with initial albuterol administration).
INDICATION: bronchospasm
CONTRAINDICATIONS: Peanut allergy, unless using nebulizer solution that does not have peanut allergen.
ADVERSE REACTIONS: Palpitations, tremors, dry mouth, tachycardia
DRUG-DRUG INTERACTIONS: sympathomimetics will further potentiate tachycardia
DOSAGE: ADULT: 0.5mg in 2.5ml NS Nebulized WITH ALBUTEROL
PEDIATRIC:
- 2-12 years: same as adult dose
- 1-2 years: 0.25mg in 2.5ml NS Nebulized WITH ALBUTEROL
CONSIDERATIONS:
- This medication is not indicated for repeat doses.
- This is only a ‘helper’ medication, and should always be given with Albuterol
Protocol 108: Calcium Chloride 10%
SCOPE: Paramedic Only
MECHANISM OF ACTION: In the cardiac myocyte, both beta blocker overdoses and hyperkalemia inactivate the critical sodium channels that are so important for the initial rush of sodium that causes depolarization of the cell, thereby leading to an action potential of electrical activity. Calcium is able to bypass the sodium channel and enhance depolarization of the cells by enhancing conduction through the L-type calcium channels. In calcium channel blocker overdoses, the increase in quantity of calcium increases the direct competitive availability of calcium in the cardiac myocyte.
ONSET: 2-5 minutes
DURATION: 30-60 minutes
INDICATION: Calcium-channel blocker overdose, beta blocker overdose, cardiac arrest associated with hypocalcemia or hyperkalemia (such as patients with end-stage renal disease)
CONTRAINDICATIONS: known hypercalcemia, digoxin toxicity, hypercalcemia
ADVERSE REACTIONS: Extravasation causes tissue necrosis, rapid administration in patients with pulses can produce a slowing of cardiac rate
DRUG-DRUG INTERACTIONS: Must be given in a separate line from IV sodium bicarbonate to prevent formation of calcium carbonate in IV line.
In presence of digitalis, may worsen cardiac output.
DOSAGE: ADULT: Not given routinely for pulseless arrest
- Pulseless arrest due to hyperkalemia, ADULT: 1gm slow IV push (over 2 minutes)
- Calcium channel blocker / beta blocker overdose: Contact MEDICAL CONTROL for approval
- Adult: 1gm slow IV/IO push, may repeat every 10 minutes for total of 3 doses
PEDIATRIC: 20mg/kg, max of 1gm slow IV/IO push (over 2 minutes) , may repeat every 10 minutes for a total of 3 doses
CONSIDERATIONS:
- Calcium GLUCONATE has similar actions but different dosages. If the ambulance service moves to purchase of Calcium GLUCONATE, this protocol does not establish dosing for that medication.
- Refer to IFT Calcium protocol for additional uses of this medication during interfacility transfers.
- Calcium chloride should NOT be used routinely in all cardiac arrests, only in those where specific indications are suspected.
Protocol 109: Dextrose / Oral Glucose
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: Delivers immediate bolus of glucose for cellular metabolism, resulting in near-immediate improvement of brain function and level of consciousness for hypoglycemic patients.
ONSET: 30 seconds
DURATION: 5-45 minutes, depending on underlying cause of hypoglycemia
INDICATION: hypoglycemia; unconscious patient with unknown etiology (if finger stick glucose unavailable or glucose monitor error)
CONTRAINDICATIONS: Hyperglycemia
ADVERSE REACTIONS: Requires a patent IV when given intravenously; extravasation leads to necrosis
DRUG-DRUG INTERACTIONS: none in the emergent hypoglycemia setting
DOSAGE:
EMT-Basic: If patient able to follow commands, give oral glucose (Glutose, 15gm oral solution)
AEMT and Paramedic:
- ADULT: 25gm IV/IO infusion
- may be given as 50 mL of a D50% solution (ampule) or 250ml of D10% solution
- PEDIATRIC: 5mL/kg of D10% solution (max of 250mL)
CONSIDERATIONS:
- attempt to draw finger stick glucose prior to administration whenever possible.
- Flush IV after use: glucose is a high irritant to veins
- May be given IO with a flush
Protocol 110: Diphenhydramine (Benadryl)
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Antihistamine used to block histamine-mediated symptoms of allergic reaction.
ONSET: 5 minutes when given intravenously; 15-30 minutes when given IM
DURATION: 3-4 hours for maximum effect, though may remain for up to 12 hours
INDICATION: allergic reaction
CONTRAINDICATIONS: acute asthma, narrow-angle glaucoma, patients taking MAO Inhibitors
ADVERSE REACTIONS: flushing, tachycardia, dilated pupils, lethargy, dry mouth, urinary retention
DRUG-DRUG INTERACTIONS:
- CNS depressants and alcohol can potentiate lethargy
- MAO Inhibitors will worsen anticholinergic effects
DOSAGE:
ADULT: 50mg IV/IO/IM
PEDIATRIC: 1mg/kg slowly over 1-2 minutes IV/IO/IM (max of 50mg)
CONSIDERATIONS:
Benadryl is sometimes used for extrapyramidal or dystonic side effects of other medications. It is sometimes combined with other medications for sedative effect. These uses require an order from MEDICAL CONTROL, and are not routinely anticipated for this medication
Protocol 111: Epinephrine
SCOPE: EMT-Basic (allergic reaction only), AEMT, Paramedic
MECHANISM OF ACTION: Epinephrine is a catecholamine that agonizes alpha, beta-1 and beta-2 receptors, causing potent vasoconstriction, elevated heart rate, myocardial contractility and bronchodilation.
ONSET: 1 minute (IV) 10-30 minutes (IM or SC)
DURATION: 5-10 minutes (IV) 30-45 min (IM or SC)
INDICATION: pulseless arrest, anaphylaxis, asthma, pediatric symptomatic bradycardia
CONTRAINDICATIONS: pulseless arrest doses (1mg) of epinephrine should not be given by IV to a patient with a pulse
ADVERSE REACTIONS: tachycardia, anxiety, angina, myocardial infarction, arrhythmias
DRUG-DRUG INTERACTIONS: None in the emergent setting; Epinephrine should not be given with sodium bicarbonate at the same time as the sodium bicarbonate will inactivate the epinephrine.
DOSAGE:
ADULT:
- (AEMT,Paramedic) Pulseless arrest: 1mg (generally 10ml of a 1:10,000 syringe) IV/IO bolus
- May repeat every 3-5 minutes. In general, should not exceed a MAXIMUM of 3 doses before contacting MEDICAL CONTROL. Contact MEDICAL CONTROL for additional doses if patient demonstrates recurrent arrest after ROSC.
- Adult Wheezing/asthma/allergic reaction: 0.3mg (1:1000) IM.
- May repeat x 1 after 15 minutes
PEDIATRIC:
- (AEMT, Paramedic) Pulseless arrest: 0.01mg/kg IV/IO (0.1ml/kg of 1:10,000 solution)
- May repeat every 3-5 minutes to a MAXIMUM of 3 doses. In general, should not exceed a MAXIMUM of 3 doses before contacting MEDICAL CONTROL. Contact MEDICAL CONTROL for additional doses if patient demonstrates recurrent arrest after ROSC.
- (Paramedic Only) Symptomatic Bradycardia: Contact MEDICAL CONTROL for authorization.
- -0.01mg/kg (0.1ml/kg of 1:10,000 solution) IV/IO
- Pediatric Wheezing/asthma/allergic reaction: 0.01mg/kg (1:1000 solution) IM (Maximum dose of 0.3mg).
- May repeat x 1 after 15 minutes.
PUSH-DOSE and “Dirty Epi Drip” Alternatives (Paramedic Only):
Shock with Cardiovascular Collapse: “Dirty Epi Drip” 1mg in 1000ml LR or NS (or 0.5mg in 500ml LR/NS) run wide open and titrate to effect.
Refractory Hypotension: as an alternative to the “Dirty Epi Drip”, dilute 1mg in 250ml or 2 mg in 500ml to create a 4mcg/ml concentration. Start infusion at 1 mcg/min (0.25ml/min) and double every 3-5 minutes, titrating to effect or maximum dose of 32mcg/min.
Push-Dose Epinephrine: as an alternative to IV drips, Push-Dose epinephrine can be invaluable, especially if needed as a ‘just in case’ option for intermittent hypotension during times patient is being off-loaded at destination facility. Mix 1 ml of 1:10,000 Epinephrine (aka “Code Epi”), in 9ml of saline. This creates a 10ml syringe with 100mcg (10mcg/ml). Administer 2-3ml (20-30mcg) every 2-5 minutes as needed to maintain hemodynamic status.
CONSIDERATIONS:
- It is extremely important to know precise dosing of both 1:10,000 and 1:1,000 preparations, particularly for pediatric patients.
- There are additional uses of epinephrine that MEDICAL CONTROL may authorize under rare circumstances, racemic epinephrine substitute, or more frequent dosing for severe anaphylaxis or adult bradycardia.
- Various combinations of drug and fluid amounts may be safely used for epinephrine drips. The 1mg/1000ml “Dirty Epi” drip ensures a ‘wide open’ flow rate would not exceed maximum safe dosage administration. Pressure infusion bags may NOT be used with this option. The 4mcg/ml concentration mix provides for ease of ‘doubling’ the dose to achieve desired effect safely, with fewest intervals between increased doses.
- Tachyphylaxis is a condition where, due to the patient’s ultimate neurologic and cardiovascular collapse, the body requires higher and higher doses of epinephrine each time it is administered to achieve the same hemodynamic effect. While not specific, it indicates a poor prognosis. When noted, this information should be provided to receiving facility of the need for increasingly higher doses.
Protocol 112: Glucagon
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: Converts stored glycogen in the liver into available sugar in the blood. Relies heavily on patient’s liver having ample storage of glycogen.
ONSET: Highly variable, 5 – 30 minutes
DURATION: Highly variable depending on patient’s available liver stores of glycogen, typically 15-30 minutes
INDICATION: Hypoglycemia with altered level of consciousness, when IV access is unavailable or anticipated to be significantly delayed
CONTRAINDICATIONS: Hyperglycemia, alert mental status (give oral glucose instead)
ADVERSE REACTIONS: tachycardia, headache, nausea and vomiting
DRUG-DRUG INTERACTIONS: None in the emergent setting
DOSAGE:
ADULT: 1mg IM
PEDIATRIC: 0.5mg IM if weight < 25kg
- 1mg IM if weight > 25kg
CONSIDERATIONS:
- This medication may be utilized for suspected beta blocker or calcium channel blocker overdoses. Contact MEDICAL CONTROL for authorization and dosing regimen.
- This medication is a ‘bridge’ medication, and is designed for TEMPORARY increase in blood glucose, which buys time to give the patient a more definitive treatment such as oral glucose, IV dextrose, or other more significant sustenance. This medication is not long-acting enough to allow for a Refusal or AMA release. As such, it is highly recommended this medication be administered while preparing the patient for transport.
Protocol 113: Ondansetron
SCOPE: EMT-Basic, AEMT, Paramedic Only
MECHANISM OF ACTION: Selective serotonin 5-HT3 receptor antagonist that results in decreased emesis.
ONSET: 1-2 minutes, peak effect in 10 minutes
DURATION: 4 hours
INDICATION: nausea and/or vomiting
CONTRAINDICATIONS: History of prolonged QT Interval
ADVERSE REACTIONS: prolonged QT interval
DRUG-DRUG INTERACTIONS: May interact with Haldol and other antipsychotic medications to prolong QT interval with fewer doses.
DOSAGE:
ADULT:
EMT-Basic: 4mg ODT PO, for ONE dose only
AEMT/Paramedic: 4mg IV/IM
- May repeat x 1 (total of 8mg) if patient is not on any other antiemetic/antipsychotic medication
PEDIATRIC > 1 year of age: Not approved for EMT-Basic
AEMT/Paramedic: 0.15mg/kg (max of 4mg) IV/IM/PO/ODT for one dose only
CONSIDERATIONS:
- In first trimester pregnancy, this medication should be used with caution, limited to one dose, and limited to use for patients with severe, intractable vomiting
Protocol 114: Phenergan
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Anticholinergic central and peripheral H-1 type histamine antagonist that results in antiemetic and sedative effects.
ONSET: 20-30 minutes (IM)
DURATION: 4-6 hours, though effects may persist up to 10-12 hours
INDICATION: Nausea and vomiting refractory to Zofran; second line agent behind Zofran; may only give first line if patient has Zofran allergy or ordered by MEDICAL CONTROL
CONTRAINDICATIONS: pediatric patients (under age 12 or less than 50kg); patients with altered mental status
ADVERSE REACTIONS: hypotension, CNS depression, confusion/altered mentation, extrapyramidal symptoms, urinary retention, agitation
DRUG-DRUG INTERACTIONS: Do not mix with other CNS depressants or anti-psychotics
DOSAGE: ADULT: 12.5mg IM only
CONSIDERATIONS:
- Drowsiness is very common, and will worsen any underlying lethargy, avoid in patients that appear altered, intoxicated, or lethargic
- Consider half dose of 6.25mg for elderly (> age 65) patients
- avoid use in pregnant patients
- Anticipate rare occurrence of dystonia and akathisia, contact MEDICAL CONTROL for consideration of treatment with benadryl
Protocol 115: Narcotic Analgesia (Fentanyl, Morphine, Dilaudid)
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Opioids target pain receptor sites, most significantly the Mu receptors in the brain and spinal cord, resulting in significant analgesia, euphoria and sedation. These also significantly increase the frequency AND severity of respiratory depression and hypotension. Morphine causes significant peripheral histamine-mediated vasodilation, increasing risk of hypotension.
ONSET: 1-2 minutes (IV)
DURATION: Fentanyl 30-60 minutes (IV), Dilaudid 1-2 hours (IV), Morphine 3-4 hours (IV)
INDICATION:
- FENTANYL and DILAUDID: Moderate to severe pain due to trauma or medical conditions.
- MORPHINE: Acute Congestive Heart Failure
CONTRAINDICATIONS: Hypotension, shock or respiratory depression
ADVERSE REACTIONS: Chest wall rigidity (fentanyl), respiratory depression and/or arrest, nausea/vomiting
DRUG-DRUG INTERACTIONS:
- Adding an opioid to a benzodiazepine has a compounding effect that greatly magnifies BOTH medications. This is considered CONSCIOUS SEDATION, and requires MEDICAL CONTROL approval.
- Opioids should be avoided in any patient that appears under the influence of alcohol, benzodiazepines, or other CNS depressants
- Avoid use with Benadryl or phenergan
DOSAGE:
FENTANYL: 0.5 – 2 mcg/kg, IN, IO or IV
may be given in 25mcg increments, especially for geriatric patient, narcotic naïve patient, or patient with low body mass index. If desired effect is achieved prior to reaching 0.5mcg/kg, the remainder of the dose does not have to be given.
dosage for adults may be rounded to closest 20mcg or 25mcg increments to allow for ease of administration.
- initial dose is generally 1 mcg/kg for medical emergencies,
- initial dose for long bone fractures should be closer to 1.5 – 2mcg/kg
- maximum of 2mcg/kg (max 200mcg adult, 100mcg < age 16, 50mcg < age 12)
- only fentanyl is approved for pediatric patients
- For transport durations greater than 30 minutes, may repeat initial dose every 30 minutes
DILAUDID: 0.5mg IV/IO only, may repeat every 15 minutes to a total of 1.5mg IV/IO
MORPHINE: 2-4 mg IV/IO, repeat x 2 every 10 minutes to a total of 10mg IV/IO
CONSIDERATIONS:
- Morphine carries significant risk of hypotension, and has no specific benefit for Acute Coronary Syndromes. Fentanyl and Dilaudid are preferred for suspected ACS, STEMI and NSTEMI cases.
- Morphine should be considered in cases of acute CHF, both to treat ‘air hunger’ and for the vasodilatory effect to shunt fluid from the lungs.
- These medications require ECG, pulse oximetry and preferably waveform capnography to be in place once administered. BLS transport may NOT be performed once pain meds have been given.
- Fentanyl is preferred in pediatric patients, and may be given IN or IV
- Consider a half dose in elderly (>60yo) patients
- Once a particular pain medication has been chosen, personnel should generally not switch to different opioid medications without discussing with MEDICAL CONTROL
Protocol 116: Benzodiazepines (Lorazepam and Midazolam)
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Benzodiazepines increase GABA activity in the brain, which is an inhibitory neurotransmitter, resulting in significant sedation, relaxant and amnestic effects.
ONSET: 1-3 minutes (IV), 5-10 minutes (IN), 15-30 minutes (IM)
DURATION: 30 minutes to 6 hours, highly dependent on patient condition and method of administration
INDICATION:
AEMT: ACTIVE tonic-clonic seizures with potential for airway compromise, - OR-
- sedation and excited delirium (in consultation with Medical Control)
Paramedic: sedation for procedural cardioversion or transcutaneous pacing, excited delirium
CONTRAINDICATIONS: hypotension, respiratory depression
ADVERSE REACTIONS: apnea, loss of airway control, bradycardia, acute delirium
DRUG-DRUG INTERACTIONS:
- Adding an opioid to a benzodiazepine has a compounding effect that greatly magnifies BOTH medications. This is considered CONSCIOUS SEDATION, and requires MEDICAL CONTROL approval.
- Adding this medication to other sedatives, such as Benadryl, Phenergan or antipsychotics may result in compounding sedation and relaxed gag reflex. This requires MEDICAL CONTROL approval.
DOSAGE:
MIDAZOLAM, ADULT:
- ACTIVE Seizure (AEMT): 2-2.5mg IV/IO or 5mg IN/IM, up to 3 doses every 2-3 minutes for status seizures.
- Sedation, Procedure or Excited Delirium:
- 2.2.5mg IV/IO or 5mg IN/IM
- For Excited Delirium, dose may be repeated up to 2 times over 10 minutes.
- Contact MEDICAL CONTROL for further dosing or alternative medication
MIDAZOLAM, PEDIATRIC:
- ACTIVE Seizure (AEMT): 0.1mg/kg, maximum of 2mg IV, up to 3 doses every 2-3 minutes for status seizures.
- IN/IM dosing is 0.2mg/kg. INTRANASAL ROUTE PREFERRED
- PR (rectal) DIASTAT may be used as alternative if prescribed to the patient
- Sedation, Procedure or Severe Agitation in a child (Paramedic): Contact MEDICAL CONTROL
LORAZEPAM, ADULT:
- ACTIVE Seizure (AEMT): 1 mg IV/IO or 2 mg IN/IM, up to 3 doses every 2-3 minutes for status seizures.
- Sedation, Procedure or Excited Delirium (Paramedic):
- 1 mg IV/IO or 2 mg IN/IM
- For Excited Delirium, dose may be repeated up to 2 times over 10 minutes.
- Contact MEDICAL CONTROL for further dosing or alternative medication
LORAZEPAM, PEDIATRIC:
- ACTIVE Seizure (AEMT): 0.05mg/kg, maximum of 1 mg IV, up to 3 doses every 2-3 minutes for status seizures.
- IN/IM dosing is 0.1mg/kg. INTRANASAL ROUTE PREFERRED
- PR (rectal) DIASTAT may be used as alternative if prescribed to the patient
- Sedation, Procedure or Severe Agitation in a child (Paramedic): Contact MEDICAL CONTROL
CONSIDERATIONS:
- CNS depression is significantly amplified when benzodiazepines are given in combination with alcohol or other benzodiazepines. It should not be done unless there are active seizures with loss of consciousness.
- All patients receiving these medications should be placed on ECG, pulse oximetry and waveform capnography.
- Once these medications are administered, these patients may not be transported without the AEMT or Paramedic as the attendant.
- Consider half doses for elderly patients (>65yo)
- Do not use these medications for pain control, except with pacing/cardioversion.
- For patients with significant agitation and altered mentation presumably due to drug use or overdose, contact MEDICAL CONTROL for dose recommendation.
- Use of these medications in conscious patients may require intubation when adverse reactions or unintended oversedation occurs due to the patient’s underlying condition. This is particularly likely in patients with significant alcohol intoxication.
Protocol 117: Lidocaine 2%
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Local anesthetic for IO infusion
ONSET: 2 – 5 minutes
DURATION: 15-45 minutes
INDICATION: pain control for IO in a conscious or disoriented patient
CONTRAINDICATIONS: allergy to anesthetics
ADVERSE REACTIONS: seizures, tachycardia, arrhythmias, hypotension
DRUG-DRUG INTERACTIONS: None in the emergent setting
DOSAGE: ADULT: 50mg slow IO push
CONSIDERATIONS:
- elderly (>65) and patients with significant CHF or liver disease are more likely to experience adverse reactions, as this medication is metabolized through the liver.
- due to lower therapeutic-to-toxic threshold of dosing, this medication is not available for pediatric (age < 12, weight < 60kg) consideration without MEDICAL CONTROL approval
Protocol 118: Magnesium Sulfate
SCOPE: Paramedic Only
MECHANISM OF ACTION: Torsades de Pointes- membrane stabilizer through stabilization of cardiac myocyte potassium channels, allowing for shortening of QT interval and correction of associated repolarization abnormalities. Asthma- while exact mechanism is uncertain, literature indicates magnesium in acute asthma acts as a weak bronchodilator with associated membrane stabilization of bronchioles.
ONSET: 10 seconds when given as a bolus for Torsades de Pointes
DURATION: 30 minutes
INDICATION: pulseless multifocal ventricular tachycardia (Torsades), asthma exacerbation refractory to other first line medications
CONTRAINDICATIONS: None in the emergent setting
ADVERSE REACTIONS: bradycardia, hypotension, respiratory depression, ‘flushed’ sensation, palpitations
DRUG-DRUG INTERACTIONS: No significant interactions that prevent use in emergent setting
DOSAGE:
ADULT- Torsades: 2gm IV/IO rapid bolus
- Refractory bronchospasm: 2gm IV/IO over 5 minutes, may administer in 100cc D5W fluid bolus
- Pediatric dosing not indicated for this medication
CONSIDERATIONS:
- This medication also has uses for pre-eclampsia and high-risk obstetrics during inter-facility transports that extend beyond the scope of this protocol. Contact MEDICAL CONTROL for any such consideration in a pre-hospital, 911 situation.
Protocol 119: Methylprednisolone
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Steroid suppression of acute inflammatory response, with secondary effect of vascular and respiratory smooth muscle relaxation.
ONSET: 1 hour
DURATION: highly variable, roughly 4-6 hours of peak effect
INDICATION: severe asthma, anaphylaxis
CONTRAINDICATIONS: Active GI bleed
ADVERSE REACTIONS: minimal in the acute single dose administration; transient hyperglycemia, agitation
DRUG-DRUG INTERACTIONS: none in the acute emergency setting
DOSAGE:
ADULT: 125mg IV/IO bolus over 2 minutes
PEDIATRIC: 2mg/kg IV/IO bolus over 2 minutes (Max 125mg)
CONSIDERATIONS:
- This is a ‘helper drug’. The purpose of giving this medication is to help the stabilization process of the acute bronchospasm. It is not a first line medication, and takes a significant time to have an effect.
- The benefit of pre-hospital administration of this medication is that is allows emergency department personnel to see if they stabilize sooner, depending on the severity of the underlying condition, providing a clearer clinical picture in a shorter period of time. It does not result in reversal of acute bronchospasm during the initial 30-60 minutes, and therefore should never be a priority to administer before other medications (oxygen, epi, albuterol, Atrovent, etc), nor should transport EVER be delayed in order to administer this on scene.
Protocol 120: Naloxone
SCOPE: EMT-B, AEMT, Paramedic
MECHANISM OF ACTION: competitive opioid receptor antagonist
ONSET: 2 – 5 minutes
DURATION: 1 – 4 hours (varies depending on type and quantity of narcotic)
INDICATION: Reverse respiratory depression associated with opioid overdose; coma of unknown etiology
CONTRAINDICATIONS: Do not give to a conscious, breathing patient. Only use if respiratory depression is present.
ADVERSE REACTIONS: tachycardia, nausea/vomiting, pulmonary edema
DRUG-DRUG INTERACTIONS: no significant interactions in the acute emergency setting
DOSAGE:
ADULT: 0.5 to 2mg IV/IO/IM/IN, repeat until reversal of respiratory depression.
- EMT-Basic: Intranasal administration is authorized
- IF respiratory arrest or airway compromise, may bolus 2 mg as initial dose
- Anticipate need for repeat doses depending on type and quantity of opioid involved
PEDIATRIC (age < 12): 0.2 mg IV/IO/IM/IN, up to 2 mg total
CONSIDERATIONS:
- Patients receiving Narcan should generally be transported to the ER for evaluation given high likelihood of recurrent CNS depression and loss of airway, or concern of other intoxicants.
- Patients who, after receiving Narcan, have the ability to demonstrate decision-making capacity, and have no concern for polysubstance abuse, alcohol intoxication, or suicidal ideation, may have the legal right to refuse transport. This should be considered and Against Medical Advice refusal, and every effort should be made to encourage transport for ER evaluation. If unsuccessful, recommend contacting MEDICAL CONTROL for attempt by the clinician to speak with the patient about the risks of recurrent CNS depression.
- When given to a patient that does NOT have respiratory depression, Narcan can potentiate sudden, severe withdrawal symptoms. This should be avoided.
Protocol 121: Nitro Sublingual
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: peripheral venous dilation that decreases cardiac preload and afterload
ONSET: 1-2 minutes
DURATION: 20-30 minutes
INDICATION: pain due to suspected MI, acute pulmonary edema due to CHF
CONTRAINDICATIONS: Hypotension, suspected Right-sided MI, erectile dysfunction medications
ADVERSE REACTIONS: hypotension, headache, syncope, sudden cardiac arrest (right side MI)
DRUG-DRUG INTERACTIONS: Cannot be mixed with erectile dysfunction medications.
DOSAGE:
ADULT: 0.4mg SL tablet every 5-10 minutes for 3 doses
- For acute pulmonary edema, MEDICAL CONTROL may order additional doses after first 3 doses
- This medication is not authorized for pediatric use
CONSIDERATIONS:
- If any evidence of hypotension or borderline hypotension, withhold this medication.
- There is evidence that supports the use of higher doses of nitro SL for acute CHF exacerbation.
- This medication protocol is considered distinct and separate from Nitroglycerin drip preparations.
- Erectile dysfunction medications have many different trade names, generic names, and increasingly more common international names as medications are ordered online from outside the U.S. If any doubt as to the type of medication, look up the medication or contact MEDICAL CONTROL before giving Nitro SL.
Protocol 122: Oxygen
SCOPE: EMT-Basic, AEMT, Paramedic
MECHANISM OF ACTION: provide additional supplemental oxygen required for cellular metabolism. Importantly, the cell of the brain do not have an anaerobic (non-oxygen) way of functioning like other parts of the body. As a result, brain cell death results in minutes without adequate oxygen.
ONSET: 1-2 minutes
DURATION: Condition dependent. Some acute respiratory conditions may desaturate as soon as high-flow oxygen is removed
INDICATION: low oxygen, chest pain, shock, anticipated airway or respiratory compromise, pre-procedural oxygenation,
CONTRAINDICATIONS: None in the emergency setting.
ADVERSE REACTIONS: None in the emergency setting (COPD-related apnea is extremely rare)
DRUG-DRUG INTERACTIONS: None in the emergency setting
DOSAGE:
- Consider use of high flow (>10lpm by NRB) for acute airway or respiratory compromise.
- For suspected stroke, intracranial hemorrhage, or acute coronary syndromes, consider only 2-4 L by NC unless there is potential for airway or respiratory compromise
- For pre-intubation preparation, use high flow dosing.
CONSIDERATIONS:
- May be used for carbon monoxide poisoning, but use high dose.
- When oxygen is indicated, so is monitoring. ECG, pulse oximetry and waveform capnography should be considered.
Protocol 123: Sodium Bicarbonate
SCOPE: Paramedic Only
MECHANISM OF ACTION: Sodium bicarb binds with hydrogen (H+) ions to form water and carbon dioxide, which helps to alkalinize the pH of the blood to further neutralize acids. It also plays a role in competitive antagonism of sodium channels during acute overdoses such as tricyclic antidepressants.
ONSET: 1-2 Minutes, but result is highly variable, depending on underlying metabolic conditions
DURATION: 8-10 minutes, depending on underlying metabolic conditions
INDICATION: Pulseless arrest suspected due to hyperkalemia (dialysis, renal disease)
- Tricyclic antidepressant overdose with hypotension or EKG evidence of widening QRS
CONTRAINDICATIONS: alkalosis, hypocalcemia, hypokalemia
ADVERSE REACTIONS: unintentional metabolic alkalosis, hypernatremia, CNS intracellular acidosis
DRUG-DRUG INTERACTIONS: AVOID GIVING WITH CALCIUM
- May decrease effectiveness of vasopressors
DOSAGE:
ADULT OR CHILDREN: 1mEq/kg slow IV push, repeated every 5 minutes up to 3 doses.
- TCA overdoses should be treated based on the QRS width. If it narrows to <100msec, hold further doses. It may require more than 3 doses to correct. In these instances, measure the QRS before and after administration, and contact MEDICAL CONTROL for further guidance.
CONSIDERATIONS:
- TCA overdoses may require larger amounts of sodium bicarbonate. At times, multiple doses may be given almost simultaneously. If the QRS is wide, consider contacting MEDICAL CONTROL early as they may guide you to treat more aggressively.
- TCA overdoses are not the only medications that cause sodium channel blockade in the heart. Other medications may result in the use of this protocol, as directed by MEDICAL CONTROL.
- Sodium Bicarb should NOT be routinely used for prolonged cardiac arrest.
Protocol 124: Furosemide
SCOPE: Paramedic Only
MECHANISM OF ACTION: As a LOOP diuretic, furosemide results in significant fluid redistribution into the urinary tract.
ONSET: 5 minutes; Peak effect at 20-30 minutes
DURATION: Up to 2 hours
INDICATION: Acute Congestive Heart Failure
CONTRAINDICATIONS: febrile (Temp >100 or infectious pattern) patients, kidney disease, hypokalemia, dialysis, hypotension
ADVERSE REACTIONS: hypokalemia, renal failure, hypotension
DRUG-DRUG INTERACTIONS: may cause significant hypotension when combined with other antihypertensives
DOSAGE: ADULT: 40mg SLOW IV push over 2-3 minutes x 1 dose only
- Not indicated for pediatric use
CONSIDERATIONS:
- Many EMS systems are removing this medication from pre-hospital use, as there is a high rate of renal complications and/or unintentional misuse in respiratory conditions that are erroneously assumed to be CHF. Before giving this medication, thoughtful consideration should be given to the likelihood of CHF and fluid overload as the principle acute cause of respiratory distress.
- Should not be given in the setting of suspected sepsis
- Should not be given if patient has a borderline or low blood pressure
- Often CHF requires multiple medications and therapies, including morphine, nitroglycerin, furosemide, CPAP, oxygen, etc. Do not consider furosemide as a solitary option in the treatment of Acute CHF.
Protocol 125: Tranexamic Acid
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: Displaces plasminogen from fibrin, resulting in inhibition of fibrinolysis, which preserves the initial clot formation. Secondarily, inhibits proteolytic activity of plasmin.
ONSET: 2-5 minutes; Peak effect at 5-10 minutes
DURATION: Up to 2 hours
INDICATION: Massive Truncal (chest, abdomen, pelvis) trauma with signs of hemorrhagic shock, including
SBP < 90mmHg or resting HR > 110bpm
CONTRAINDICATIONS: not approved for pediatric < age 12, suspected CVA, MI, PE or hypersensitivity to medication
ADVERSE REACTIONS: hypotension, nausea/vomiting, blurry vision, clot formation, seizures
DRUG-DRUG INTERACTIONS: no acute drug interactions in the emergent setting
DOSAGE: ADULT: 1 gram administered over 10 minutes, mixed in 100ml of Normal Saline
- A second dose of 1 gram administered over 10 minutes may be administered if no hypersensitivity is noted after the first dose
- Not indicated for pediatric use
CONSIDERATIONS:
- This protocol was developed with input from the Centura Trauma System’s medical direction and with consideration towards standards of care identified in the Rural Trauma Team Development Course, from the American College of Surgeon’s Committee on Trauma.
- Patients with an identified hypercoagulable state should receive only the initial dose, then contact MEDICAL CONTROL
- The use of this medication requires signs of significant internal bleeding, including but not limited to unstable vitals, altered LOC, and mechanism of truncal traumatic injury.
- This medication is not approved for routine non-traumatic use, but may be ordered by MEDICAL CONTROL for certain life-threatening medical indications such as postpartum or post-operative hemorrhage.
Protocol 126: Ketamine
SCOPE: Paramedic Only
MECHANISM OF ACTION: Ketamine is a dissociative anesthetic agent, structurally similar to phencyclidine (PCP). At low doses it provides analgesia, at higher doses it produces amnesia and sedation. It’s therapeutic side effects include beta-adrenergic stimulation, including an increase in blood pressure (beta-1 agonist) and bronchodilation (weak beta-2 agonist).
ONSET: 45-60 seconds; Peak effect at 3-5 minutes
DURATION: Up to 1 hour
INDICATION: induction for rapid sequence intubation, analgesia for severe trauma, sedation for maintenance of intubation with or without mechanical ventilation
CONTRAINDICATIONS: known hypersensitivity; penetrating eye trauma; severe hypertension (>200 SBP, >120 DBP), tachyarrhythmias
ADVERSE REACTIONS: laryngospasm, vomiting, hypersalivation, severe emergence reaction (awaken with hallucinations), jaw trismus
DRUG-DRUG INTERACTIONS: no acute drug interactions in the emergent setting
DOSAGE:
ADULT:
- Induction: 1-2 mg/kg IV
- Maintenance after Induction: 0.25-0.5 mg/kg IV every 5-10 minutes
- Agitation/excited delirium: 4mg/kg IM. Ensure access to airway at all times regardless of restraints.
- Analgesia for major trauma:
- 50mg IM or IntraNASAL, repeat every 30 minutes as needed
- 20mg slow IO or IV, repeat every 20 minutes as needed
PEDIATRIC:
- Induction/maintenance: contact Medical Control
- Analgesia for major trauma:
- 0.5-1 mg/kg IM or IN, repeat every 30-40 minutes as needed
- 0.1-0.3 mg/kg slow IO or IV, repeat every 20-30 as needed
CONSIDERATIONS:
- Excited delirium is a condition where the patient is in acute psychosis and cannot make rational decisions, requiring a combined approach by EMS and law enforcement to, at times, restrain the patient for the sake of their safety and the safety of the crew. In these instances, a higher dose of IM injection is used that can result in airway compromise, jaw trismus, and respiratory arrest. It is always advisable to involve Medical Control as soon as possible in the decision to administer this medication for this condition.
Protocol 127: Haloperidol
SCOPE: Paramedic Only
MECHANISM OF ACTION: Antipsychotic medication that blocks dopamine receptors, resulting in sedation and tranquilization. Secondary effects include a mild alpha-adrenergic blockade, peripheral vasodilation, and QT prolongation.
ONSET: 2-5 minutes IV; 10 minutes IM; Peak effect at 5-10 minutes IV, 30 minutes IM
DURATION: Up to 2-4 hours
INDICATION: Severe agitation, combative patient, significantly combative intoxicated patient unable to refuse due to lack of mental capacity.
CONTRAINDICATIONS: suspected acute MI, hypotension, respiratory or CNS depression, pregnancy
ADVERSE REACTIONS: hypotension, tachycardia, QT prolongation, restlessness, hyperactivity or anxiety. Rare instanced of neuroleptic malignant syndrome (high fever with muscular rigidity). Extrapyramidal reactions including spasm of muscles of tongue, face, neck and back (this may be treated with IV Benadryl).
DRUG-DRUG INTERACTIONS: Avoid combination with other QT prolonging antipsychotics and antiemetics (Zofran).
DOSAGE: ADULT: 5-10mg IM. Use a half dose in patients whose age are > 65.
- Contact Medical Control for administration to patients under the age of 16.
CONSIDERATIONS:
- May combine with Benadryl, and either Ativan or versed (if EtOH is not suspected), but should be done with extreme caution and cardiac/airway monitoring.
- Ideal for use with intoxicated patients who should not receive benzodiazepines.
Protocol 128: Rapid Sequence Intubation Medications
SCOPE: PARAMEDIC ONLY. (Note: This protocol is not the procedure protocol, it only lists the medication considerations, order of administration and dosages for RSI.)
- SEDATE first- choose one of the following, use IDEAL Body Weight for estimated dosing:
- Etomidate 0.3mg/kg IV/IO, or
- Etomidate 0.1mg/kg IV/IO (if concern for potential hypotension), or
- Ketamine 1.5mg/kg IV/IO (recommended for asthma or unstable, hypotensive patients), or
- Midazolam (Versed) 0.2-0.3mg/kg IV/IO (Max 10mg), or
- (Adults Only) Fentanyl 50mcg PLUS Versed 2-2.5mg IV/IO
- Paralyze last- choose one of the following, use IDEAL Body Weight for estimated dosing:
- Avoid paralysis if suspected diabetic ketoacidosis
- Succinylcholine 1-2mg/kg IV/IO
- Rocuronium 1 mg/kg IV/IO
- Vecuronium 0.15-0.2mg/kg IV/IO
- Long-Term Sedation and Paralysis
- Sedation
- Midazolam 2.5mg IV/IO every 5-10 minutes as needed
- Ketamine 0.25-0.5mg/kg IV/IO every 10-15 minutes as needed
- Pain Management
- Fentanyl 1mcg/kg IV/IO every 30 minutes as needed
- Ketamine 20mg-30mg IV/IO every 30 minutes as needed
- Paralysis (if patient attempting to self-extubate)
- Rocuronium 1mg/kg IV/IO every 45-60 minutes as needed
- Vecuronium 0.1mg/kg IV/IO every 45-60 minutes as needed
- Sedation

Protocol 129: Toradol
SCOPE: AEMT, Paramedic
MECHANISM OF ACTION: NSAIDs like Toradol decrease pain by inhibiting cyclooxygenase enzymes, thereby blocking prostaglandin production. This reduces overall inflammation and swelling (which is often a cause of pain).
ONSET: 5 minutes; Peak effect at 60 minutes
DURATION: Up to 4 hours
INDICATION: Acute treatment of moderate or severe pain due to suspected kidney stones, chronic pain or musculoskeletal pain.
CONTRAINDICATIONS: allergies to NSAIDs or aspirin, pregnancy, GI bleeds, kidney disease, bleeding disorder or taking anticoagulant medication, acute head injury, age less than 16 or greater than 65 years, severe dehydration.
ADVERSE REACTIONS: allergic reactions, vomiting, GI bleeds, worsening kidney injury
DRUG-DRUG INTERACTIONS: do not administer with any other NSAIDs or anticoagulants
DOSAGE: ADULT (Age 16 or greater for this medication): 15mg IV or IM x 1 dose
Not approved for pediatric patients under age 16.
CONSIDERATIONS:
- Generally it is best to avoid this medication with patients who present with extreme tenderness in the abdomen that may require surgery (eg appendicitis or cholecystitis).
- This medication should not be used in patients with acute truncal trauma.
Protocol 130: Neosynephrine or Phenylephrine
SCOPE: EMT-Basic, AEMT, and Paramedic
MECHANISM OF ACTION: Alpha-adrenergic vasoconstrictor. When administered intranasally, it vasoconstricts superficial blood vessels in the nasal mucosa, reducing the degree of bleeding and swelling.
ONSET: 2-5 minutes; Peak effect at 5-10 minutes
DURATION: 1-2.5 hours
INDICATION: epistaxis, nasal intubation
CONTRAINDICATIONS: none
ADVERSE REACTIONS: rare if given intranasally
DRUG-DRUG INTERACTIONS: no acute drug interactions in the emergent setting
DOSAGE:
ADULT: First, have patient blow nose to expel clots, then administer two sprays into each nostril
- Not indicated for pediatric use
CONSIDERATIONS:
- Avoid accidental spray into the eyes.
- This medication is often most effective when used in combination with nasal clamp after medication has been administered.
Protocol 131: Flumazenil (Romazicon)
SCOPE: AEMT and Paramedic
MECHANISM OF ACTION: Flumazenil is a selective GABA receptor antagonist that reverses the effects of benzodiazepines.
ONSET: 30-60 seconds; Peak effect at 5-10 minutes
DURATION: 30-50 minutes
INDICATION: oversedation for ventilator management with signs of hypotension, severe benzodiazepine overdose (requires Medical Control approval first)
CONTRAINDICATIONS: avoid in patients with known seizure disorders; because the risk of irreversible seizures is always a significant concern, it may be more appropriate to provide supportive treatment and ventilatory support while benzodiazepines are metabolized by the body.
ADVERSE REACTIONS: cardiac dysrhythmias, prolonged seizures, aspiration, hypoxia, vomiting
DRUG-DRUG INTERACTIONS: this medication blocks the effects of anti-seizure medications, especially benzodiazepines that would be used to correct a seizure.
DOSAGE:
ADULT:
For suspected benzodiazepine overdose on 911 scene, contact Medical Control first.
- Typical dose is 0.2mg IV/IO over 15-30 seconds, repeated once every 1-2 minutes up to a maximum dose of 1mg IV/IO.
- For adverse reaction to administered benzodiazepine: 0.2-0.4mg IV/IO once.
- Paramedic Only: For oversedation on ventilatory support: in absence of hypotension or bradycardia, do not administer flumazenil. If oversedation presents with accompanying circulatory system problems, administer 0.2-0.4mg IV/IO once. May repeat every 1-2 minutes until resolution of complications up to a maximum of 2mg, taking care to keep ventilated patient sedated appropriately.
CONSIDERATIONS:
- There is a high risk of seizures with the administration of this medication. “Start low (dose), go slow (with repeat dosing)”. Remember, this medication BLOCKS the medications typically used to stop seizures. Therefore, in the event of a flumazenil-induced seizure, the normal anti-seizure medications will not work, and airway problems can become significantly prolonged, resulting in hypoxic brain injury.
- In general, if there is a concern of mixture of opiates and benzodiazepines, it is strongly preferred that Narcan be administered up to at least 2mg before considering this medication.
- If a patient requires intubation or a supraglottic airway for polypharmacy overdose (eg alcohol and benzodiazepines), it is generally best to place the airway and provide ventilatory support, and avoid use of flumazenil until evaluated in the emergency department. In this instance, flumazenil should be reserved for patients with hypotension and/or failure to ventilate successfully with BVM +/- a supraglottic airway.
Protocol 132: Acetaminophen
SCOPE: EMT-Basic, AEMT, and Paramedic
MECHANISM OF ACTION: Acetaminophen metabolizes to p-aminophenol, which can cross the blood-brain barrier where it acts on brain and spinal tissue at COX and opioid receptor sites, to lower fever and decrease pain.
ONSET: Approximately 30 minutes
DURATION: Up to 6 hours
INDICATION: Fever, pain
CONTRAINDICATIONS: Liver failure, known sensitivity
ADVERSE REACTIONS: nausea, vomiting, Stevens-Johnson Syndrome, headache, anxiety, dyspnea, fatigue,
DRUG-DRUG INTERACTIONS: No acute interactions; chronic Tylenol use can interact with blood thinners and/or lead to liver toxicity.
DOSAGE: Adult: 325mg to 1,000mg, may repeat every 6 hours.
- Pediatric or Alternative Adult dosing, weight-based: 10-15mg/kg every 4-6 hours.
CONSIDERATIONS:
- Acetaminophen is an ingredient in most combination pain medications (Norco, Vicodin, Percocet) and over-the-counter cold preparations. The total maximum 24 hr dose should not exceed 4 grams in an adult when all acetaminophen components are added together.
Protocol 201: Initial BLS Airway
Scope: EMT-Basic, Advanced EMT and Paramedic
INDICATIONS:
- Unable to respond to commands
- Loss of consciousness
- airway compromise
- sonorous (“snoring”) respirations
- cardiac arrest
CONTRAINDICATIONS:
- able to respond to commands
- intact gag reflex is a contraindication to oral pharyngeal airway
- facial fractures are a contraindication to a nasal pharyngeal airway
PROCEDURE:
- Open the airway
- Medical: jaw thrust/chin lift
- Trauma: modified jaw thrust
- Visually EXAMINE the open airway
- Evaluate for swelling/edema, blood, teeth, vomitus
- Suction any fluid/blood
- AVOID suction if edema/swelling
- If evidence of solid obstruction, proceed to Obstructed Airway protocol
- Identify Mallampati Airway Score
- Mallampati ONE = all structures visualized, space between uvula and tongue
- Mallampati TWO= all structures visualized, no space between uvula and tongue
- Mallampati THREE= only a portion of uvula visualized, soft palate still visible
- Mallampati FOUR= uvula not visualized; soft palate not fully visualized, tonsils not visualized
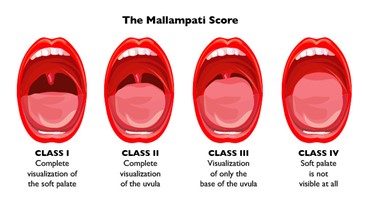
Mallampati Score
- Insert oral pharyngeal airway (OPA)
- Measure from corner of mouth to tip of ear lobe for proper size
- Insert at 90 degree or 180 degree to glossus, rotating as it is seated in posterior pharynx
- If gag reflex present, switch to lubricated nasopharyngeal airway (NPA)
- Measure from TIP of NOSE to tip of ear lobe
- NPA should be inserted perpendicular to back of head, not in line with nare
- If resistance, switch to other side
- If unsuccessful on both sides, maintain manual airway opening
- Avoid in facial fractures or with signs of basilar skull fracture
- VISUALLY CONFIRM NPA extends past base of tongue in posterior pharynx
- If patient is unable to maintain their own airway, and condition does not permit OPA or NPA, the following options should be considered depending on the clinical context:
- Manual maintenance of jaw thrust/chin lift
- Insertion of supraglottic rescue airway device (eg King or iGel)
- Lateral recumbent positioning
- Request Paramedic response for advanced airway
- Once airway is secured with BLS airway device, attach high-flow oxygen by mask
- If patient is unable to maintain effective ventilation rate, VENTILATE with BVM
- Ventilation rate is 12-20 for adults
- Ensure tight seal around mouth/nose, may require two-handed technique for difficult airway
- VENTILATE with supplemental O2 attached as soon as possible
- If patient demonstrates some respiratory effort that is not adequate to sustain life, support breaths with BVM ventilation during inhalation effort (ie ‘poor man’s CPAP’ technique)
- If still unable to ventilate despite all above efforts, declare a “FAILED AIRWAY”
- Rapid transport to ER, notifying ER of failed airway
- Paramedic intercept if available
CONSIDERATIONS:
- The higher the Mallampati score (3 or 4) the more likely the airway is to be difficult to manage. Consider moving to more advanced airway maneuvers sooner, or dedicating two people to effective BVM seal/technique.
- The sound of SNORING means AIRWAY OBSTRUCTION due to the TONGUE. Take action NOW!!!
- A “FAILED AIRWAY” is a critical emergency that requires rapid transport, ALS intercept and early ER notification.
- Some situations may require recurrent / near-continuous suction, such as GI bleed, posterior epistaxis, dental bleeding, etc.
- A Cervical Collar DOES NOT maintain airway in jaw thrust position. If Manual jaw thrust is necessary, maintain manually IN ADDITION to the cervical collar.
- Brain cells die quickly without glucose and oxygen, beginning within several minutes. Permanent brain death begins in less than 4-6 minutes without effective oxygen. Therefore, GOOD BLS AIRWAY management is vital to prevention of permanent anoxic brain injury during initial response.
Protocol 202: Intubation, Oral
Scope: Paramedic Only
INDICATIONS:
- Respiratory Failure
- Absence of airway reflexes
- Airway obstruction
CONTRAINDICATIONS:
- Pediatric airway successfully ventilated with BLS measures
- Presence of airway (“gag”) reflexes
- Multiple failed intubation attempts (see “Failed Airway” protocol)
- In cardiac arrest, initial resuscitation efforts of chest compressions, BLS ventilation and defibrillation should occur before attempts to secure an advanced airway
TECHNIQUE:
- Initiate BLS airway procedure, to include ventilation and pre-oxygenation.
- Identify Mallampati Airway Score of patient to assist with determination of a difficult airway
- If Mallampati grade 3 or 4, no more than 2 attempts should be made to intubate before placing an alternative supraglottic ‘rescue’ airway device
- Identify possible traumatic factors:
- If trauma considerations are present, assign in-line spinal stabilization prior to intubation attempt
- If no evidence of trauma, position towards the ‘sniffing position’, of neck flexion and head extension. May consider cervical hyperextension as an alternative depending on airway visualization.
- Perform direct laryngoscopy. If unable to visualize glottic structures, consider use of Selleck’s maneuver or adjustment of laryngoscope backwards.
- ONLY once glottic structures are visualized, place endotracheal tube.
- Most adult females will require ETT size 6.5 - 7.5.
- Most adult males will require ETT size 7.0 - 8.0.
- Size pediatric ETT based on weight- or height- based measurements (eg Broselow tape).
- MARK tube depth after visualization of ETT balloon through cords and inflation of balloon.
- Confirm ETT placement with continuous waveform capnography. Additional supporting documentation may include:
- Symmetry of breath sounds
- Tube condensation
- Improving SpO2
- Ventilate with Bag-Valve-Mask.
- Continue monitoring during transport with continuous waveform capnography, reassessing tube placement, oxygenation and ventilation.
- If patient declines after intubation, consider “DOPE”:
- Dislodgement
- Obstruction
- Pneumothorax
- Equipment failure
CONSIDERATIONS:
- Hyperventilation is generally not indicated for most intubated patients.
- It is strongly recommended to print a copy of EtCO2 at arrival to ER to document tube placement before transfer to ER.
- Personnel qualified to intubate must be capable of assessing the anticipated level of airway difficulty utilizing the Mallampati Airway Score.
Protocol 203: Intubation, Nasal
Scope: Paramedic Only
INDICATIONS:
- Age 12 (or > 50kg) or older, spontaneously breathing patient requiring airway protection that cannot tolerate laryngoscopy
- Airway obstruction
- Wired or clenched jaw in patient requiring airway protection (eg status seizures)
- Lack of airway reflexes
- Failed ventilatory effort with CPAP/BiPAP or BVM.
CONTRAIDICATIONS:
- Apnea (nasal intubation requires spontaneous respirations)
- Facial trauma
- Anticoagulated patients with significant risk of epistaxis
- Effective ventilations with BVM
TECHNIQUE:
- Initiate BLS airway procedure, to include ventilation and pre-oxygenation.
- Identify possible traumatic factors:
- If trauma considerations are present, assign in-line spinal stabilization prior to intubation attempt
- If no evidence of trauma, position towards the ‘sniffing position’, of neck flexion and head extension. May place the patient in upright, seated position if situation permits.
- ETT size is dependent on ability to fit through nare, though size should be as close as possible to the size the patient normally would need for oral intubation.
- Lubricate tube and consider application of lidocaine jelly if available. Stylet should NOT be used for this procedure.
- Attach Beck Airway Airflow Monitor (BAAM) device or similar adjuvant.
- With head in midline position, advance tube through the largest nare to posterior pharynx. STOP if any significant resistance is met.
- Continue to advance with steady pressure, listening for confirmatory ‘whistle’ of BAAM device. Wait for inspiratory effort before passage through cords. Anticipate slight resistance as tube passes vocal cords.
- Advance an additional 2cm, inflate cuff, confirm with BAAM, waveform capnography and symmetry of breath sounds.
- Secure tube.
- Ventilate with BVM at appropriate rate.
- Transport with ETT monitored under waveform capnography.
- If patient declines after intubation, consider “DOPE”:
- Dislodgement
- Obstruction
- Pneumothorax
- Equipment failure
CONSIDERATIONS:
- Hyperventilation is generally not indicated for most intubated patients.
- It is strongly recommended to print a copy of EtCO2 at arrival to ER to document tube placement before transfer to ER.
- Whenever possible, if patient can be successfully ventilated using CPAP/BiPAP or BVM, it is recommended to refrain from blind nasotracheal intubation.
- Positioning of the patient and gentle, constant pressure are key to this procedure. Advancing the tube requires patience and confirmation with BAAM-type auditory confirmation device.
Protocol 204: Cricothyrotomy
Scope: Paramedic Only
INDICATIONS:
- Life-threatening airway obstruction requiring endotracheal airway management, unable to successfully ventilate by any means (including BVM and/or CPAP/BiPAP) AND endotracheal intubation has failed or cannot be performed due to obstruction.
- Remember the phrase “cannot intubate or ventilate”.
CONTRAINDICATIONS:
- Age less than 12.
- Able to ventilate with BVM, CPAP/BiPAP or other airway positioning maneuver.
TECHNIQUE:
- The preferred technique for surgical cricothyrotomy is “Cut-Finger-Bougie-Airway”
- Position the patient supine, with neck extended if no traumatic considerations.
- Identify landmarks of thyroid and cricoid cartilage; stabilize the larynx with one hand as a “tracheal ‘hug’”.
- CUT- Using a scalpel, make a 3cm vertical incision through the skin and fascia over the cricothyroid membrane. Then puncture the cricothyroid membrane, twisting the scalpel 180 degrees to open up the membrane for passage of a tube.
- FINGER- Bluntly dissect the tissue with small fingertip, ensuring access through the cricothyroid membrane.
- BOUGIE- Insert the bougie curve-tip through the incision, sliding down towards the patient’s lower airway.
- AIRWAY- Advance 6-0 tracheal tube over the bougie and into the trachea. Keep firmly seated while removing the bougie.
- Secure the airway and inflate the balloon.
- Initiate ventilation with a BVM and high-flow oxygen.
- Confirm placement with waveform capnography, symmetrical breath sounds, and pulse oximetry.
CONSIDERATIONS:
- While the above procedure is preferred, if a bougie is not available, a tracheal hook may be utilized to lift the cricoid cartilage and provide counter-traction during placement of the tracheal tube.
- In rare instances, a horizontal incision may be needed after identifying the cricothyroid membrane to extend the area for appropriate advancement of the tracheal tube.
- Consider this a procedure where you ‘see’ with your finger, not your eyes. The membrane must be accurately identified by feeling the anatomical landmarks. As bleeding occurs, especially in the presence of a traumatic event to the face/jaw, it will be very difficult to visualize the passage.
- There is a HIGH rate of failure of this procedure, even when trained and performed properly, due to false passages created where the tube goes to the side of, or above, the cricothyroid membrane. Observe closely for subcutaneous emphysema, low pulse oximetry, poor EtCO2 or poor lung sounds.
- If procedure fails, ventilate as best as possible, and transport rapidly to closest available facility. NOTIFY DESTINATION HOSPITAL of failed cricothyrotomy so they may prepare rapid interventions on arrival.
- This procedure requires periodic skill check-offs by the Medical Director on at least an annual basis.
Protocol 205: Pediatric Needle Cricothyrotomy
Scope: Paramedic Only
INDICATIONS:
- A life-threatening condition exists AND adequate oxygenation and ventilation cannot be accomplished by other less invasive means for patients < 12 years old.
CONTRAINDICATIONS:
- If patient can be ventilated and oxygenated by less invasive means.
PROCEDURE:
- Ensure patent upper airway with placement of an oral airway and nasal airway, unless contraindicated.
- Open pre-prepared kit, attach angiocath to syringe, and aspirate 1-2 mL of saline into syringe
- Prepare skin using aseptic solution
- Insert the IV catheter through the skin and cricothyroid membrane into the trachea. Direct the needle at a 45° angle caudally (toward the feet). When the needle penetrates the trachea a “pop” will be felt.
- Aspirate with the syringe. If air is retuned easily or bubbles are seen (with saline), the needle is in the trachea.
- Advance the catheter over the needle while holding the needle in position, then withdraw needle after catheter is advanced flush to skin.
- Remove the plunger and attach the 3 mL syringe to the catheter hub
- Attach the 15 mm adaptor to the syringe chamber
- Oxygenate the patient with bag-valve-mask device using the 15 mm adaptor provide high flow oxygen.
- Confirm and document catheter placement by:
- Waveform capnography
- Pulse oximetry
- Do not let go of catheter and be careful not to kink the catheter. There is no reliable way to secure it in place, and it is only a temporizing measure until a definitive airway can be established at the hospital
- Observe for subcutaneous air, which may indicate tracheal injury or extra- tracheal catheter position
- Continually reassess oxygenation and catheter position.
CONSIDERATIONS:
- Needle cricothyrotomy is a difficult and hazardous procedure that is to be used only in extraordinary circumstances as defined below. The rationale for this procedure must be documented in the patient care report.
- Due to the funnel-shaped, rostral, highly compliant larynx of a pediatric patient, cricothyrotomy is an extremely difficult procedure to successfully perform. As such, every effort should be made to effectively oxygenate the patient before attempting needle cricothyrotomy.
- A standardized, pre-prepared kit is recommended, and can be assembled using common airway equipment. An example is given below. Kit selection may vary and should be approved by the individual agency Medical Director.
EXAMPLE OF KIT:
- 18 ga. (Infants and Children) and 16 ga. (Adolescent/Adult) catheter over needle
- 3 mL syringe
- 15 mm (3.0-3.5 ET) endotracheal tube adaptor that fits the 3 mL syringe
Protocol 206: Supraglottic Airway (King LT or iGel)
Scope: EMT-Basic, Advanced EMT and Paramedic
INDICATIONS:
- Designated advanced airway for EMT/AEMT
- Rescue airway if unable to intubate
- Difficult airway (Mallampati 3 or 4), may be used as primary airway if intubation anticipated to be difficult in setting of respiratory failure requiring rapid airway control
- Preferred advanced airway in pediatric patients
- Should be utilized after two failed attempts at endotracheal intubation by most experienced provider on scene
CONTRAINDICATIONS:
- Intact gag reflex
- Caustic (acid/base) ingestion
- Severe maxillofacial trauma
- Appropriate size airway not available
- Unresolved airway obstruction
- Relative Contraindication: esophageal varices with active hematemesis (consider contacting Medical Control first)
PROCEDURE/APPROACH:
- Initiate BLS Airway sequence
- Select proper size airway
- For King LT:
- Test balloon
- Ensure proper size syringe for full inflation
- Lubricate distal tip
- Maximize oxygenation with BVM ventilations, and suction if indicated
- Position:
- If atraumatic: sniffing position or slight cervical hyperextension
- If trauma: maintain neutral position with in-line spinal stabilization
- Insert airway, may hold tongue manually to mandible to assist with passage around posterior glottis
- For King LT: Inflate balloon with full volume of air
- Confirm Placement: Auscultate and ventilate
- Confirm lung sounds
- EtCO2
- Monitor:
- Waveform capnography if available is gold standard for monitoring
- SpO2
- Vitals q 5 minutes
- 3 Lead ECG for all intubated/advanced airway patients
- Complications: Remember acronym DOPE for complications with advanced airways:
- D: Dislodged Tube
- O: Obstruction (mucous plugs, vomit, blood, etc)
- P: Pneumothorax
- E: Equipment Failure (BVM, lack of O2, cuff failure)
CONSIDERATIONS:
- All personnel need to be familiar with appropriate sizing of airways, and the type of airway (King LT, iGel, etc) used by the agency.
- Do not remote a functioning supraglottic airway to attempt intubation unless the clinical concern is specifically related to vocal cords/glottic condition
- Use with caution in patients with broken teeth, which may lacerate balloon

Protocol 207: CPAP
SCOPE: EMT-Basic, AEMT, Paramedic
INDICATIONS:
- Symptomatic patients with moderate-to-severe respiratory distress as evidenced by at least two (2) of the following:
- Rales (crackles), rhonchi, or wheezes
- Dyspnea with hypoxia (SpO2 less than 90% despite O2)
- Dyspnea with inability to speak full sentences
- Accessory muscle use
- Respiratory rate greater than 24/minute despite O2
- Diminished tidal volume.
CONTRAINDICATIONS:
- Respiratory or cardiac arrest
- Systolic BP less than 90mmHg
- Lack of airway protective reflexes
- Significant altered level of consciousness such that unable to follow verbal instructions or signal distress
- Vomiting or active upper GI bleed
- Suspected pneumothorax
- Trauma
- Patient size or anatomy prevents adequate mask seal
PROCEDURE: Generic
- Place patient in a seated position and explain the procedure to him or her
- Assess vital signs (BP, HR, RR, SpO2, and ETCO2)
- Apply the CPAP mask and secure with straps, progressively tightening as tolerated to minimize leaks.
- Operate CPAP device according to manufacturer specifications.
- Start with the lowest continuous pressure that appears to be effective.
- Adjust pressure to achieve the most stable respiratory status
- Monitor patient continuously, record vital signs every 5 minutes.
- Assess patient for improvement as evidenced by the following:
- Reduced dyspnea
- Reduced verbal impairment, respiratory rate and heart rate
- Increased SpO2
- Stabilized blood pressure
- Appropriate ETCO2 values and waveforms
- Increased tidal volume
- Observe for signs of deterioration or failure of response to CPAP:
- Decrease in level of consciousness
- Sustained or increased heart rate, respiratory rate or decreased blood pressure
- Sustained low or decreasing SpO2 readings
- Rising ETCO2 levels or other ETCO2 evidence of ventilatory failure
- Diminished or no improvement in tidal volume
SEE APPENDIX --- FLOWSAFE 2 EZ Application
SEE APPENDIX --- Zoll Ventilator Application
PROCEDURE: FLOWSAFE 2 EZ
- Connect O2 tubing nipple to gas source
- With Nebulizer in off position, slowly increase gas flow to 6 or 8 LPM
- Adjust flowmeter until desired pressure is obtained.
- DO NOT EXCEED 30 LPM
- Black ports on mask allow additional O2 administration if required
If Nebulizer is Needed
- Apply medication to nebulizer and assure clear O2 line is attached.
- Adjust flowmeter to obtain desired CPAP pressure. (up to 25LPM may be required)
DIAGRAMS BELOW ARE FOR GENERAL REFERENCE.
THESE INCLUDE GENERIC LPM VS CPAP PRESSURE, O2 TANK TIME CHART AND CPAP NEBULIZED MEDICATION GUIDELINES



PROCEDURE: ZOLL VENTILATOR
- Open vent Circuit
- Attach ribbed vent tubing to large silver orifice, Green tubing to green flared fitting, Clear tubing to silver fitting.
- Connect O2 line direct to Ambulance Main O2 via DISS Quick connect or attach to D or E cylinder valve via DISS port.
- Attach Viral filter to back of exhalation tube.
- Apply Mask to patient secure with straps, progressively tightening as tolerated to minimize leaks
- Turn on Zoll Ventilator, Select CPAP.
- Vent will default to 5 of PEEP
- Adjust FiO2 to 100.
- Apply Vent Circuit to CPAP mask
- Adjust PEEP as needed
CONSIDERATIONS:
- Should patient deteriorate on CPAP:
- Troubleshoot equipment
- Consider endotracheal intubation
- Assess need for possible chest decompression due to pneumothorax
- Assess for possibility of hypotension due to significantly reduced preload from positive pressure ventilation
- Some fixed pressure CPAP devices do not have FiO2 adjustment and will only administer up to 30% oxygen. If no improvement in oxygenation with a fixed pressure CPAP device, consider adding supplemental oxygen.
- If exposure precautions are advised, utilize viral filter between mask and vent circuit as well as covering patients head with towel due to possible mask leaks if tolerated.
Protocol 208: Needle Decompression
Scope: Paramedic ONLY
INDICATIONS:
- All of the following indicators must be present:
- Severe respiratory distress
- Hypotension or signs of shock
- Unilateral absent or decreased breath sounds
- Consider bilateral needle chest decompression in traumatic pulseless arrest if patient is being resuscitated in presence of any truncal trauma
- Consider bilateral needle decompression in patients with respiratory distress and significant chest wall trauma (eg ejection from vehicle, gun shot wound, stab wounds)
CONTRAINDICATIONS:
- Pneumothorax, without evidence of tension, distress or signs of shock
PROCEDURE/APPROACH:
- Expose the entire chest.
- Time permitting, clean skin overlying site with available prep
- Insert catheter at 2nd intercostal space at midclavicular line, or 5th intercostal space at midaxillary line.
a. Either approach is acceptable, generally the site with the least soft tissue overlying ribs is preferred
b. For adult, use largest (10ga or 14ga, 3 inch catheters), longest available angiocath
c. For smaller children under age 12, shorter angiocath is appropriate
d. Leave in place for approximately 30 seconds, then remove needle, leaving catheter in place
4. Notify receiving hospital of needle decompression.
CONSIDERATIONS:
- In the rural setting with the possibility of extended transport times, a repeat decompression should be considered if indications present the need.
- Angiocath may become occluded with blood or by soft tissue. If patient presents with recurring symptoms, do not assume the catheter is still working just because it is in the chest wall. If recurring symptoms, it is reasonable to remove and repeat procedure.
- A simple pneumothorax is NOT an indication for needle decompression.
- Extra care is needed when performing on a pediatric patient.
Protocol 209: Intraosseous Needle Placement
Scope: Advanced EMT and Paramedic
INDICATIONS:
- Primary vascular access device when peripheral IV not obtainable in patient with critical illness
- Unable to obtain IV access in patients with cardiopulmonary arrest or impending arrest
- Profound shock with severe hypotension and poor perfusion
- May use as first line access for emergent or unconscious conditions including: status seizures, airway compromise, trauma with significant mechanism or concern for threat to primary survey
CONTRAINDICATIONS:
- Fracture of target bone or area more proximal to target bone
- Cellulitis of skin overlying insertion site
- Osteogenesis imperfecta (rare condition predisposing to fractures with minimal trauma)
- Total knee replacement (hardware will prevent placement)
PROCEDURE/APPROACH:
- Site of choice- proximal tibia or humeral head.
- Either drill or manual insertion may be performed at either of these sites.
- Select appropriate size IO needle relative to the insertion site. For EZ-IO:
a. Blue size for tibial insertion
b. Yellow size for humeral head insertion
c. Pink size for pediatric tibial insertion
4. Clean skin per agency approved aseptic technique.
5. Place intraosseous needle perpendicular to the bone.
6. Follow manufacturer’s guidelines specific to the device being used for insertion.
7. Entrance into the bone marrow is indicated by sudden loss of resistance.
8. Flush line with 10ml saline
a. IO infusion is very painful. If the patient is conscious, administer lidocaine per protocol for pain control before infusing fluids or medications.
9. Secure IO and IV line.
a. Even if properly placed, the needle will not be secure. The needle must be secured and the IV tubing taped. The IO needle should be stabilized at all times.
b. A person should be assigned to monitor the IO at the scene and en route to the hospital.
10. Observe for signs of limb swelling or decreased perfusion to distal extremity that would indicate a malpositioned IO catheter, compartment syndrome or other complication. If limb becomes tense or malperfused, disconnect IO tubing immediately and leave IO
in place.
11. In general, it is preferred to only make one attempt per bone, unless emergent circumstances require repeat effort.
12. Do not remove IO needles in the field.
13. Notify hospital staff of all insertion sites/attempts.
CONSIDERATIONS:
- The glenohumeral head site is ideal for rapid infusion of blood products, fluids and medications, and can flow at the same rate as an 18ga angiocath in the antecubital site.
- Avoid starting a tibial IO in a leg with suspected hip, femur or ankle fracture.
- If multiple IVs are needed (eg massive trauma) it is reasonable to consider multiple IOs.
- IOs are faster and require less prep/securing time than IVs, and should be frequently considered for trauma activations with suspected or impending shock (eg trauma Red patients).
- If the drill fails, may use manual technique to insert an IO.
Protocol 210: Tourniquet
Scope: EMT-Basic, Advanced EMT, Paramedic
Indications:
- Life threatening extremity hemorrhage.
- Limb amputation with hemorrhage.
Contraindications:
- Non-extremity hemorrhage
- Proximal extremity location where tourniquet application is not practical (See Junctional TQ)
Procedure/Approach:
1. If unable to control hemorrhage using direct pressure, apply tourniquet according to manufacturer specifications and using the steps below:
a. If unable to quickly and easily ascertain the location of the bleed, apply the tourniquet as “HIGH and TIGHT” as possible on the limb.
b. If able to quicky determine location of the bleed, apply the tourniquet 2-3 inches proximal to the wound, but not across any joints. If bleed is within 2 inches of a joint, apply above the joint.
c. Removal of clothing is optional before applying a tourniquet: if life-threatening exsanguination is occurring, a tourniquet may be applied immediately without exposing the site to prevent blood loss.
2. Tighten tourniquet until bleeding stops. Applying tourniquet too loosely will only increase blood loss by inhibiting venous return.
3. If bleeding is not controlled with the application of a single tourniquet, a 2nd can be applied adjacent to the 1st.
4. Mark the time and date of application.
5. If there is concern for sliding/movement of the tourniquet it is appropriate to secure or wrap the tourniquet with an ace bandage or medical tape to prevent slippage.
6. Keep tourniquet on throughout transport to the hospital – a correctly applied tourniquet should only be removed by the receiving hospital.
7. Dress wounds per standard wound care protocol.
Considerations:
- “Rule of 2/3rds”: Two-thirds of lower extremity amputations and/or blast injuries to lower extremities often require TWO OR MORE tourniquets to stop arterial hemorrhage. Do not delay in applying additional tourniquets. Apply UNTIL BLEEDING STOPS.
- Checking distal pulses is not warranted in these circumstances. Do not waste time assessing distal perfusion, as it should not be there if tourniquet is truly effective.
- The time frame for considering removal of tourniquets, or ‘dressing down’ tourniquets in a disaster or tactical setting is 2 hours. If transport to a hospital destination is delayed by this length of time, contact MEDICAL CONTROL for consideration of
removal/dressing down the tourniquet. Otherwise, leave it in place.
Protocol 211: Pelvic Binder
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Instability of the pelvis due to trauma
- Significant traumatic mechanism involving pelvis
- Significant perineal/genital trauma
- Lower extremity amputation due to explosive trauma or ejection from vehicle
Contraindications:
- Impaled object that prevents application of binder
- Uncontrolled lower junctional bleed
Procedure/Approach:
1. Commercial pelvic binder should be applied per the manufacturer’s specification.
2. Device should always be applied around the greater trochanters (below the belt line, not above).
3. Improvised pelvic binders may be used if a commercial binder is not available, to include:
a. Sheet wrapped around lower pelvis
b. Vacuum body splint applied with pressure applied to trochanters as splint is hardened
c. In absence of the above, may consider inward rotation of feet/knees to upright position and taping the knees and toes together. This inward rotation moves the greater trochanters inward toward the pelvis, applying additional pressure to the intended
area.

Considerations:
- Application of pelvic binding is best considered as a treatment concept, not a specific tool or device. A commercial binder is ideal, but can fail during transport or frequent movement. All personnel should be familiar with alternative improvised pelvic binders in
the event of equipment failure.
- The application of a pelvic binder is a critical intervention to prevent internal bleeding in the pelvis and is standard for Pre-hospital Trauma Life Support, Advanced Trauma Life Support, and Tactical Combat Casualty Care standards. The early application of
this device has been shown to save lives and should be considered early in any high-mechanism truncal trauma.
- If there is not a pelvic fracture, the application of a pelvic binder will not cause damage. When in doubt, apply the binder.
Protocol 212: Junctional Hemorrhage
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- The need to stop life-threatening bleeding in the area of an extremity/ joint close to the trunk of the patient where a standard tourniquet would not be applicable.
Contraindications:
- None, in the setting of acute junctional bleeding
Procedure/Approach:
- Direct pressure to the wound, use fingers and hands to apply pressure to the area to control bleeding. May apply pressure more proximally if arterial control can be achieved at key pressure points (eg iliac artery).
- Remove clothing to expose wounds/ injuries. Try to maintain constant direct pressure.
- Consider Hemostatic Dressing (Quikclot): This must be placed first during the wound packing process to properly work.
- Begin packing the wound with Z-fold dressing. Use fingers to push dressing into place and fill the cavity. Be prepared to add a significant amount of additional packing until you have a firm ball of packing that extends outside the wound, for the junctional tourniquet to be placed on. This can often require up to ten (10) rolls of gauze, unrolled and ‘belt-fed’ into the wound with constant, firm pressure.
- Use SJT (Sam Junctional Tourniquet) to stop bleeding if necessary. Check pulses in extremities to confirm proper placement of SJT. Note time when SJT is applied with your initials.
Considerations:
- Never remove the dressings to check if bleeding has stopped.
- When using SJT over top of a wound apply extra dressings to the area.
- The SJT can also be used as a pelvic binder.
- When using SJT for axillary hemorrhage, use the strap that comes with SJT. Also, use the included SJT extender (This is needed due to subclavian vessels lying deeper in the body.) See manufacturer application recommendations.
- Commercial junctional tourniquets commonly fail due to lack of adequate packing of the wound prior to application, or due to positional slippage. They must be constantly monitored during movement and transport, similar to how closely you would monitor an advanced airway device.
- Improvised junctional tourniquets may be used with proper training and approval from the medical director. These are valuable to learn as not all junctional locations can be reached with the SJT or other commercial junctional tourniquets.
- The proper application of these wound dressings is manpower intensive. It typically requires a minimum of one person to hold constant pressure, with a second packing the wound and applying the tourniquet.
Protocol 213: Synchronized Cardioversion
Scope: Paramedic ONLY
Indications:
- Unstable tachyarrhythmia with a pulse
Contraindications:
- Hemodynamically stable patients should be managed medically when possible
- Pulseless patient
- Heart rate less than 150 (adults) or 180 (children)
Technique:
- Prepare for cardioversion
- High-flow oxygen
- IV access
- Airway and suction equipment prepared and ready
- Sedate with benzodiazepine
- Print 12 lead prior to cardioversion
- Perform Cardioversion
- Synchronize prior to charging (see manufacturer instructions for monitor)
- Charge for appropriate dose
- Adult: 200 Joules biphasic
- Pediatric: 0.5-1 Joules/kg biphasic
- Print post-cardioversion 12 lead
- If no change, or rhythm rapidly returns to baseline tachyarrhythmia, reassess vitals and contact MEDICAL CONTROL for further guidance.
Considerations:
- If it appears to be a regular, narrow complex tachyarrhythmia, consider trial attempt of adenosine prior to cardioversion.
- Consider the “H’s and T’s” of ACLS: attempt to identify the cause of the arrhythmia, as sometimes cardioversion will not correct the arrhythmia until the underlying cause is addressed, especially for cases of Atrial Fibrillation with Rapid Ventricular Response.
- Patients in Atrial Fibrillation that are NOT anticoagulated pose a high risk of clot formation in the heart that, after cardioversion, can result in a stroke. Consider contacting MEDICAL CONTROL in these instances before cardioversion.
- If cardioversion is successful, be prepared to see ‘reperfusion arrhythmias’ for a short period of time. Reassess vitals, mental status and patient symptoms, and refrain from repeat cardioversion. These rarely require any further intervention.
Protocol 214: Transcutaneous Pacing
Scope: Paramedic ONLY
Indications:
- Unstable bradycardia
- Unresponsive with bradycardia
- Symptomatic A-V blocks
Contraindications:
- Asymptomatic bradycardia with otherwise normal vital signs
- Pacing is rarely indicated in patients under the age of 12 years
- Pulseless arrest
Procedure/Approach:
- Apply appropriate multi-function pads (adult vs pediatric) per manufacturer guidelines
- Set pacing mode to 1:1
- Set pacing rate to 80
- Start milliamp (mAmp) setting at Zero.
- Turn pacer on, ensure pacing artifact markings are appropriately positioned pre-systole.
- Slowly increase the milliamps approximately 10 mA every 10-15 seconds while observing ECG for capture (usually between 40 – 100 mA)
- Once electrical capture occurs, confirm with manual pulse check
- If no capture occurs with maximum output (usually 200 mA), discontinue pacing and resume ACLS.
Considerations:
- May consider sedation with benzodiazepine for pain associated with electrical pulsations if blood pressure permits
Protocol 215: Rapid Sequence Intubation
Scope: Paramedic ONLY
Indications:
- GCS < 10 with airway compromise
- Airway compromise due to obstruction, swelling or injury
- TBI or CVA with unconsciousness with intact gag reflex
- Combative with inability to maintain airway, after ruling out hypoglycemia
- Trismus of jaw
- Respiratory failure with intact gag reflex
Contraindications:
- Any patient that can be oxygenated and ventilated by less invasive means
- Age < 12 or small enough to measure on Broselow tape
- Known allergy to RSI medications
Procedure/Approach:
- PREPARE the patient
- Preoxygenate the patient with high flow oxygen via BVM
- Suction, intubation and rescue airway devices ready
- IV or definitive glenohumeral IO must be established for RSI protocols
- Evaluate Mallampati classification
- Note landmarks for cricothyrotomy
- Routine or prophylactic pre-medication with lidocaine or atropine is no longer recommended unless there is a clear indication for consideration of these medications
- SEDATE first- choose one of the following, use IDEAL Body Weight for estimated dosing:
- Etomidate 0.3mg/kg IV/IO, or
- Etomidate 0.1mg/kg IV/IO (if concern for potential hypotension), or
- Ketamine 1.5mg/kg IV/IO (recommended for asthma or unstable, hypotensive patients), or
- Midazolam (Versed) 0.2-0.3mg/kg IV/IO (Max 10mg) or
- (Adult Only) fentanyl 50mcg PLUS Versed 2-2.5mg IV/IO
- Paralyze last- choose one of the following, use IDEAL Body Weight for estimated dosing:
- Avoid paralysis if suspected diabetic ketoacidosis
- Succinylcholine 1-2mg/kg IV/IO
- Rocuronium 1mg/kg IV/IO
- Vecuronium 0.15-0.2mg/kg IV/IO
- Perform Endotracheal Intubation
- Cricoid pressure may be used to visualize vocal cords
- If successful, verify placement with waveform EtCO2, pulse ox and lung sounds
- If unsuccessful after 2 attempts, go to Failed Airway protocol
- Long-Term Sedation and Paralysis
- Sedation
- Midazolam 2.5mg IV/IO every 5-10 minutes as needed
- Ketamine 0.5mg/kg IV/IO every 10-15 minutes as needed
- Pain Management
- Fentanyl 1mcg/kg IV/IO every 30 minutes as needed
- Ketamine 20mg-30mg IV/IO every 30 minutes as needed
- Paralysis (if patient attempting to self-extubate)
- Rocuronium 1mg/kg IV/IO every 45-60 minutes as needed
- Vecuronium 0.1mg/kg IV/IO every 45-60 minutes as needed
- Ventilation
- A sedated and paralyzed patient may be placed on a ventilator for transport to the ER provided the paramedic has completed the Medical Director’s RSI Training Program.
- The safest default is to continue with BVM attached to supplemental oxygen.
- Sedation
Considerations:
- In general, when preparing RSI in presence of a rotary wing flight team on scene, defer to the flight team as the higher standard of care. They should take charge of medication decisions once at the side of the patient.
- Performance of this procedure as a Standing Order requires completion of the Medical Director’s RSI Training Program and annual competency check-off, otherwise it requires approval from Medical Control.
- This procedure is ideally performed when the paramedic has either a second medic or advanced EMT available to assist with the multiple steps of airway management.
- There is a significantly lower success rate of RSI in patients with a complex airway (Mallampati grade 3 or 4).
- RSI is not recommended when able to maintain SpO2 > 90% by less invasive means.
Protocol 216: Physical Restraints
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
Patient that poses physical danger to him/herself or others that fails verbal de-escalation attempts including, but not limited to:
- An impaired patient (illicit drug use, injury or illness) that lacks decision-making capacity regarding his/her care
- A violent, combative or non-communicative patient that won’t engage in verbal de-escalation
- A suicidal patient on a mental health hold at risk for dangerous behavior to his/herself or others
Contraindications:
- EMS personnel may not utilize handcuffs. Those are to be placed by law enforcement and transported with law enforcement escort.
- In situations where it is unsafe without law enforcement, personnel should withdraw from the scene and await sufficient law enforcement personnel before attempting placement of restraints
- Prone positioning is never permitted with restraints.
Procedure/Approach:
- Attempt to verbally de-escalate the patient.
- Prepare all equipment and personnel, including restraints and assignments (generally 1 rescuer per limb plus one for the torso and one for the head).
- Attempt to explain what needs to be done and why. Any small success at getting the patient to voluntary get on the pram will make the placement of restraints much easier.
- In general, all four extremities should be placed in restraints to fully protect the patient from falls and to protect the provider from assault.
- Patient should be restrained in supine or seated position, with one arm above the head, one arm down by the side of the patient. This prevents the ability to roll into an unsafe position or sit up violently and rip through restraints or head butt responders.
- Reassess: patient’s airway, limb circulation and vital signs.
- Document rationale for restraints, efforts taken to de-escalate prior to restraints, any adverse events or injuries, and reassessment of the patient.
Considerations:
- Whenever possible, law enforcement should be present and available to assist.
- Chemical restraints may be used per Agitated/Combative Patient Protocol and medication protocols in concert with physical restraints, provided patients are monitored on heart monitor, as well as vital signs and continuous airway reassessment.
Protocol 217: Stoma/Tracheostomy Suctioning
Scope: Advanced EMT and Paramedic
Indications:
- Tracheostomy with debris or thick mucous hindering respiratory effort.
Contraindications:
- None.
Procedure/Approach:
- Measure approximate length of soft tip suction catheter from stoma/tube to 2nd ICS or roughly 2cm below the sternal notch.
- Remove T-tube if a tracheostomy patient is on humidified oxygen.
- Insert soft-tip suction catheter into opening with suction off (or thumb-hole of suction catheter uncovered).
- Initiate suction as catheter is slowly removed, but no longer than 10 seconds.
- If mucous plugs or thick secretions are present, 3-5 ml of sterile saline may be slowly flushed through the stoma/tracheostomy to loosen or thin the secretions. Sterile saline may also be nebulized to assist with loosening mucous plugs or secretions.
Considerations:
- Loose, bleeding or infected stomas or tracheostomies should be treated cautiously. Any fluid draining into the airway may require active suction, but may limit the depth at which the catheter is placed, to limit stimulation of coughing and/or inhalation of draining fluid. Therefore, any suction of fluid/blood/pus occurring at or near the skin level should be done by placing the suction tip just at the immediate site of drainage, and not deeper into the airway.
Protocol 301: Failed Airway
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Patient unable to maintain their own airway
- Airway compromise is determined to be the principle life threat
- Two failed intubation attempts by most proficient provider
- Three total failed intubation attempts
- Poor SpO2 (<85%) with BVM/adjuncts alone
Contraindications:
- Adequate ventilation/oxygenation with BLS interventions
- Cardiac Arrest
Procedure/Approach:
- Consider cause of failed airway
- Paramedic only: If due to significant gag reflex, seizure or jaw rigidity: Contact Medical Control to request authorization for Rapid Sequence Intubation
- Assign two personnel to airway for two-hand assisted BVM for better seal
- Attach HIGH FLOW OXYGEN
- Consider repositioning head/neck/jaw thrust
- Consider adjuncts based on gag reflex and oxygenation:
- OPA
- NPA
- King Airway
- Declare “We are Working a Failed Airway” over radio
- Initiate Emergent Transport As Soon As Possible
- Enables Paramedic Intercept if one not present on scene
- Notifies ER of incoming emergent airway
- Paramedic Only: If ventilation remains inadequate and upper airway obstruction/mechanism is suspected, consider Cricothyrotomy
Considerations:
- This protocol is intended for use only when Airway compromise is considered the principle life threat. The intent is to focus the entire EMS team on the fact that the airway requires management by ER providers beyond what is available on scene, and therefore transport should be expedited.
- Cellular death of the brain begins almost immediately after SpO2 drops. Within 4 minutes, irreparable harm to the brain is caused.
- Once a “Failed Airway” is declared, all other interventions should be initiated during transport to the hospital.
- In a cardiac arrest, multiple aspects of emergency care are being performed simultaneously, including CPR, ECG rhythm recognition, airway management, defibrillation and medication administration. In cardiac arrest, the other aspects of emergency care should not be pushed aside for rapid transport solely for airway management.
Protocol 302: Obstructed Airway
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Suspected upper airway obstruction
Contraindications:
- Patient able to speak or productively cough
Procedure/Approach:
- If patient is unconscious, initiate chest thrusts
- Open airway, and look for foreign body to remove, then,
- attempt ventilation with BVM
- If unsuccessful, repeat chest thrusts until obstruction relieved
- If unable to clear despite several rounds of chest thrusts, initiate “Failed Airway” protocol
- Paramedic Only: If unable to ventilate, perform laryngoscopy
- McGill forceps may be used to either remove or push object out of way
- Consider cricothyrotomy
- Once obstruction is relieved consider:
- lateral recumbent positioning
- High flow oxygen
- Suction as needed
- Ventilation with BVM to support respirations
- If patient is conscious,
- If productively coughing or speaking do NOT initiate maneuvers
- If evidence of partial obstruction, consider:
- Position of comfort
- High-flow oxygen
- Suction as needed
- If patient deteriorates, refer back to step 1) “If patient is unconscious”
- If evidence of partial obstruction, consider:
- If signs of severe chocking (silent, stridor, cyanosis)
- Initiate Heimlich maneuver immediately until obstruction cleared or patient becomes unconscious
- For visibly pregnant patients, perform chest thrusts
- For infants, alternate between 5 chest thrusts and 5 back blows
- If patient deteriorates, refer back to step 1) “If patient is unconscious”
- If productively coughing or speaking do NOT initiate maneuvers
Considerations:
- Certain medical conditions may appear as upper airway obstruction but may not be a ‘foreign body’. These include, but are not limited to anaphylaxis, familial hereditary angioedema, epiglottitis, inflammatory angioedema, medication-related angioedema. In these instances, chest thrusts/Heimlich have no value.
- Conscious infants will typically scream/cry once object has been dislodged. If there is absence of noise in a conscious infant, assume alternating chest thrusts/back blows should continue.
Protocol 303: Adult Respiratory Distress
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Initial evaluation of all acute respiratory distress in adults
Contraindications:
- Trauma-related respiratory complaints
- Airway obstruction -> Obstructed Airway Protocol
Procedure/Approach:
- While evaluating causes, initiate supplemental oxygen
- Obtain vital signs, including mental status, ECG, SpO2, and waveform capnography
- If respiratory rate / depth insufficient to sustain life, assist ventilations with BVM
- Consider the following causes of respiratory distress:
- Pulmonary embolism -> Rapid Transport
- Pneumonia -> Sepsis Protocol
- Allergy / Anaphylaxis -> Anaphylaxis Protocol
- Acute MI -> Chest Pain and/or Cardiac Alert Protocol
- Spontaneous Pneumothorax
- Sepsis -> Sepsis Protocol
- Acidosis -> Consider Hyperglycemia / DKA Protocol
- Anxiety -> Psychiatric Patient Protocol
- Congestive Heart Failure -> CHF Protocol
- COPD Exacerbation
- Asthma Attack -> Adult Wheezing Protocol
- Consider use of CPAP for suspected acute CHF, asthma or COPD exacerbation
- Consider use of albuterol in suspected asthma, COPD or allergic etiology
- Obtain a 12 Lead ECG
- Obtain large bore (20g or greater) peripheral IV at or above antecubital site
- If potentially unstable or in clear distress, initiate Rapid Transport
- Paramedic Only: consider Rapid Sequence Intubation if respiratory failure appears imminent (eg decreased GCS score, poor SpO2, ineffective ventilations)
Considerations:
- As much as possible, avoid requesting rapid sequence intubation from medical control for cases of suspected acidosis (eg diabetic ketoacidosis) as paralysis will often result in sudden cardiac arrest.
- A printout of waveform capnography is extremely valuable in the evaluation of undetermined respiratory distress. Waveform capnography is the “EKG of Ventilation”
Protocol 304: Pediatric Respiratory Distress
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Initial evaluation of all acute respiratory distress in children under age 12
Contraindications:
- Trauma-related respiratory complaints
- Airway obstruction -> Obstructed Airway Protocol
Procedure/Approach:
- While evaluating causes, initiate supplemental oxygen
- Obtain vital signs, including mental status, ECG, SpO2, and waveform capnography
- Evaluate positioning (are they in a tripod position?) and expose chest to evaluate accessory muscle use
- If respiratory rate / depth insufficient to sustain life, assist ventilations with BVM
- Neonate – typical rate 40/min
- Infant- typical rate 30/min
- Toddler to Elementary School age- typical rate 20/min
- Consider the following causes of respiratory distress:
- Stridor (‘bark’ like cough) -> Pediatric Upper Airway Stridor Protocol
- Allergy / Anaphylaxis -> Anaphylaxis Protocol
- Acidosis -> Consider Hyperglycemia / DKA Protocol
- Asthma Attack -> Pediatric Wheezing Protocol
- Consider use of albuterol in suspected asthma
- Consider epinephrine in suspected acute allergic/anaphylaxis
- Obtain peripheral IV
- Check temperature for suspected febrile illness
- If potentially unstable or in clear distress, initiate Rapid Transport and contact Medical Control as soon as possible
Considerations:
- As much as possible, avoid requesting rapid sequence intubation from medical control for cases of suspected acidosis (eg diabetic ketoacidosis) as paralysis will often result in sudden cardiac arrest.
- A printout of waveform capnography is extremely valuable in the evaluation of undetermined respiratory distress. Waveform capnography is the “EKG of Ventilation”
- A leading cause of pediatric stridor is foreign body ingestion/aspiration
- Time permitting, request vaccination history from parents for suspected infectious etiology
Protocol 305: Adult Wheezing
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- History and exam consistent with bronchospasm (expiratory wheezing)
Contraindications:
- Divert to Congestive Heart Failure Protocol if they appear fluid overloaded
- Divert to Anaphylaxis Protocol if evidence of allergic etiology
- Consider Adult Respiratory Distress Protocol for critical interventions if evidence of respiratory failure
- Trauma- related respiratory complaints
- Airway Obstruction -> Obstructed Airway Protocol
Procedure/Approach:
- Administer oxygen, assess SpO2 and waveform capnography
- Establish IV access
- Obtain 12 Lead EKG
- Administer nebulized albuterol and ipratropium (Atrovent)
- May give continuous albuterol nebulizer for severe distress/bronchospasm
- Ipratropium should only be given once
- Consider CPAP early if evidence of significant labored breathing, inability to speak
- If CPAP is contraindicated or unavailable, may assist ventilation with BVM
- Administer methylprednisolone
- Do not delay transport for administration of this medication- it works over several hours and will not resolve the condition quickly
- Paramedic Only: If patient does not respond to the above treatment modalities:
- Consider IV magnesium
- Consider IM epinephrine if no concern for current or prior coronary artery disease
Considerations:
- IM Epinephrine should generally not be used for wheezing related to COPD, or in patients with cardiac history. It should be reserved for patients who present consistent with severe asthma or allergic considerations.
- At times this protocol may overlap with the Adult Respiratory Distress Protocol, especially in elderly COPD patients with multiple medical problems. These protocols are not exclusive of one another. They may be combined in settings of complex patient presentations, especially if they present in imminent respiratory failure. Do not hesitate to contact Medical Control with any questions or concerns.
- Solu-Medrol (methylprednisolone) works well to prevent hospitalization in moderate asthma, but does not work like a ‘rescue’ medication. It takes several hours to work. While EMS administration of this medication is helpful to speed up the disposition of the patient from the ER, it does not have an immediate impact. Transport to the ER should be prioritized over IV administration of this medication in situations of acute respiratory distress.
Protocol 306: Pediatric Wheezing
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Wheezing in patients less than 16 years of age
Contraindications:
- Trauma-related respiratory complaints
- Airway obstruction -> Obstructed Airway Protocol
Procedure/Approach:
- Begin initial approach of Pediatric Respiratory Distress Protocol
- In general, pediatric wheezing should always be transported to the ER for assessment by a clinician.
- Determine age of patient:
- Age < or = 2 years old, more likely to be bronchiolitis than asthma
- Oxygen is most important priority, titrate to > 90%
- May consider suction of nostrils with 3ml saline if significant secretions
- May trial a dose of albuterol.
- If improvement is seen with albuterol, contact Medical Control for consideration of steroids and/or ipratropium.
- If no improvement with albuterol, transport to ER.
- Age > 2, more likely to be reactive airway disease, such as asthma
- After oxygen has been initiated, consider administration of either MDI or nebulized albuterol, per medication protocols.
- May use patient’s MDI if present.
- May repeat for a total of 3 doses.
- May give as a continuous nebulizer for severe respiratory distress.
- AEMT / Paramedic -> consider addition of one dose of ipratropium.
- If severe exacerbation, or worsening respiratory distress,
- Consider IM epinephrine 0.01mg/kg
- Initiate a peripheral IV or IO
- Consider IV Solu-medrol, 2mg/kg
- Initiate fluid bolus of 20ml/kg
- Consider BVM assist with ventilations for severe respiratory distress
- Initiate Rapid Transport and early notification of ER
- After oxygen has been initiated, consider administration of either MDI or nebulized albuterol, per medication protocols.
- BLS Airway is the preferred airway in pediatric patients.
- Age < or = 2 years old, more likely to be bronchiolitis than asthma
Considerations:
- Bronchiolitis is the most common cause of wheezing in children under 2 years of age. Typically it is characterized by a fever, secretions and distress. It is most common in the winter months, and is best treated with supplemental oxygen, suction and transport.
- Asthma typically presents over 2 years of age, of over 1 year in patient with strong family history. Observe for accessory muscle use, tripod positioning, pursed lips, prolonged expiration. Prior history of similar symptoms is important to discern from the parents.
- Waveform capnography gives an accurate picture of reactive airway disease (asthma) when the presentation is unclear or there is a lack of history. Consider early application of capnography prior to initiation of albuterol / ipratropium, and continue to monitor resulting changes after treatment.
- While bronchiolitis and asthma are the most common causes of wheezing, consider the following possibilities as well: traumatic chest injury, croup, epiglottitis, pneumonia, congenital heart disease, anaphylaxis, DKA, sepsis, or foreign body.
- Solu-medrol does not take effect fast enough to help pre-hospital course of the illness. The purpose of EMS administering this medication is to lessen the time for moderate / severe asthma to stabilize while they are in the ER, thereby speeding the decision making for discharge vs hospitalization. Transport should never be delayed because of administration of solu-medrol alone.
Protocol 307: Congestive Heart Failure
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Shortness of breath with rales or pitting bilateral lower leg edema
- Adults with history of CHF with respiratory complaint
Contraindications:
- Trauma-related respiratory complaints
- Adults with body-wide edema (anasarca) or significant history of liver cirrhosis with known ascites
Procedure/Approach:
- Begin initial approach of Adult Respiratory Distress Protocol
- Obtain 12 Lead, rule out acute MI / STEMI pattern
- Consider Nitroglycerin, 0.4mg sublingual, up to 3 doses
- If oxygenation / ventilation is inadequate, initiate CPAP
- If inadequate response to CPAP, consider BVM assist with ventilation
- Initiate Rapid Transport and early ER notification
- Lasix, 40mg, may be considered in known CHF patients currently taking Lasix.
- If patient mental status declines, contact Medical Control for consideration of advanced airway options
Considerations:
- Morphine should not be used in suspected CHF.
- Nitroglycerin is preferred over diuretics (Lasix) to pull fluid from the lungs into the preload / vena caval system.
- This is an optional medication for the agency to carry, depending on supply and demand of other medical treatment options.
Protocol 308: Medical Cardiac Arrest
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Atraumatic cardiac arrest in adolescents or adults (> age 12)
Contraindications:
- Traumatic arrest
Procedure/Approach:
- Initiate BLS resuscitation
- Start CPR
- May use autopulse device for appropriately sized patients if immediately ready,
- otherwise start chest compressions first, then set up autopulse device per manufacturer recommendations
- Apply AED and shock if indicated
- Repeat AED check every 2 minutes
- Initiate oxygen therapy with ventilations
- Start CPR
- If AEMT or Paramedic on scene:
- Attach manual defibrillator
- Shockable Rhythm (VF/VT)
- Defibrillate, then immediate 2 min of CPR
- IV / IO access
- Epinephrine 1mg IV/IO q 3-5 min
- Defibrillate, then immediate 2 min of CPR
- Amiodarone 300mg IV/IO, may repeat with 150mg once after 3-5 min if refractory VF/VT
- Defibrillate, then immediate 2 min of CPR
- Place Advanced Airway
- Torsades de Pointes -> Magnesium Sulfate 2gm IV/IO
- Not Shockable Rhythm (Asystole/PEA)
- Immediate 2 min of CPR
- IV / IO access
- Epinephrine 1mg IV/IO q 3-5 min
- Reassess for Shockable Rhythm
- Place Advanced Airway
- PACING IS NOT INDICATED IN ASYSTOLE OR PEA
- Shockable Rhythm (VF/VT)
- Attach manual defibrillator
- CONSIDER REVERSIBLE CAUSES and Treatment Alternatives
- Hydrogen Ion Acidosis -> Sodium Bicarb 1mEq/kg IV/IO once
- Hypovolemia -> Fluid Bolus, at least 500cc pressure infusion
- Hypokalemia -> Contact Medical Control
- Hyperkalemia -> Calcium Chloride 1 gm IV/IO over 2 minutes
- Hypoglycemia -> 1amp D50 IV/IO
- Hypothermia -> active rewarming (“never dead until ‘warm and dead’”), transport
- Hypoxia -> supplemental oxygen with ventilation
- Toxins -> Contact Medical Control
- Tamponade, Cardiac -> Contact Medical Control
- Tension Pneumothorax -> Needle Decompression
- Thrombosis, Coronary or Pulmonary -> Contact Medical Control
- Trauma -> Bilateral Needle Decompression, Rapid Transport
- If Return of Spontaneous Circulation (ROSC) -> Post-Cardiac Arrest with ROSC Protocol
- If prolonged asystole without ROSC for > 30 min, consider Termination of Resuscitation -> Field Pronouncement Protocol
Considerations:
- Follow current ACLS guidelines for chest compressions, ventilation ratios and quality of CPR
- In general, Calcium Chloride should not be given unless clear history (eg dialysis, potassium overdose) of causative factors for hyperkalemia exist.
- In general, it is in the patient’s best interest to have full ACLS resuscitation immediately on scene as opposed to immediate transport. By providing ACLS measures on scene, you ‘bring the ER to the patient’ and do everything the ER can do, only you are able to do it earlier in the timeline. This creates the best chance for survival.
- In general, once a supraglottic airway demonstrates successful oxygenation and ventilation, intubation should be avoided to allow the team to focus on other efforts.
Protocol 309: Pediatric Cardiac Arrest
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Atraumatic cardiac arrest in children < age 12
Contraindications:
- Traumatic arrest
Procedure/Approach:
- Initiate BLS resuscitation
- Start CPR
- Follow current AHA BLS and PALS guidelines for chest compressions
- Minimize interruptions, resume compressions immediately after shocks or rhythm checks. Check pulses only if organized rhythm.
- Apply AED with pediatric pads and shock if indicated
- Repeat AED check every 2 minutes
- Initiate oxygen therapy with ventilations
- Start CPR
- If AEMT or Paramedic on scene:
- Attach manual defibrillator
- Shockable Rhythm (VF/VT)
- Defibrillate, 1st shock at 2J / kg, then immediate 2 min of CPR
- IV / IO access
- Epinephrine 0.01mg/kg (or may use Broselow tape) IV/IO q 3-5 min
- Defibrillate, 2nd shock at 4J / kg, then immediate 2 min of CPR
- Amiodarone 5mg/kg IV/IO ONCE, then contact MEDICAL CONTROL for further dose consideration
- Defibrillate, 3rd shock at 4J / kg, then immediate 2 min of CPR
- BLS airway is preferred, focus care on high quality CPR
- Torsades de Pointes -> extremely rare in pediatric patients, contact Medical Control as Magnesium Sulfate is not indicated in pediatric patients per PALS guidelines.
- Not Shockable Rhythm (Asystole/PEA)
- Immediate 2 min of CPR
- IV / IO access
- Epinephrine 0.01mg/kg (or may use Broselow tape) IV/IO q 3-5 min
- Reassess for Shockable Rhythm
- BLS airway is preferred, focus care on high quality CPR
- PACING IS NOT INDICATED IN ASYSTOLE OR PEA
- Shockable Rhythm (VF/VT)
- Attach manual defibrillator
- CONSIDER REVERSIBLE CAUSES and Treatment Alternatives
- Hydrogen Ion Acidosis -> Sodium Bicarb 1mEq/kg IV/IO once (or may use Broselow Tape)
- Hypovolemia -> Fluid Bolus, 20cc/kg (or may use Broselow tape)
- Hypokalemia -> Contact Medical Control
- Hyperkalemia -> Contact Medical Control
- Hypoglycemia -> D10 bolus IV/IO
- Hypothermia -> active rewarming (“never dead until ‘warm and dead’”), transport
- Hypoxia -> supplemental oxygen with ventilation
- Toxins -> Contact Medical Control
- Tamponade, Cardiac -> Contact Medical Control
- Tension Pneumothorax -> Needle Decompression
- Thrombosis, Coronary or Pulmonary -> Contact Medical Control
- Trauma -> Bilateral Needle Decompression, Rapid Transport
- If Return of Spontaneous Circulation (ROSC) -> Post-Cardiac Arrest with ROSC Protocol
- In General, all pediatric cardiac arrest without obvious signs of death should be transported to the ER.
Considerations:
- Follow current AHA BLS and PALS recommendations for compressions and ventilation ratios.
- Generally, BLS airway management is preferred unless intubation is required for specific indications, such as obstruction, inability to ventilate with BVM, etc.
- Utilize EtCO2 to measure for abrupt return in ROSC
Protocol 310: Neonatal Resuscitation
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Preterm infant in respiratory failure
- Neonate (<30 days old) in cardiopulmonary failure
Contraindications:
- None
Procedure/Approach:
- The following interventions should occur in the first 30 seconds of assessment:
- Warming
- Clear Airway if necessary
- Dry
- Stimulation (actively stimulate with vigorous rubbing of back)
- Evaluate ABCs:
- If > 100 bpm and no respiratory distress or apnea, continue routine care
- If < 100 bpm, Labored breathing, cyanosis or apnea à supplemental oxygen therapy
- Reassess airway
- Consider ventilation for apnea or bradypnea
- If < 60 bpm, START CHEST COMPRESSIONS
- Ventilate with positive pressure and supplemental oxygen
- Reassess after 60 seconds
- AEMT or Paramedic:
- if no improvement in heart rate after 1 minute of resuscitation, consider epinephrine IV/IO
- Consider IV fluid bolus
Considerations:
- Mild peripheral cyanosis at birth does not always indicate need for resuscitation. Newborn infants generally do not require resuscitation if they:
- Are full term gestation
- Crying or breathing
- Have good muscle tone
- CPR should follow standard AHA BLS for Healthcare Providers guidelines
- 2 thumbs-encircling hands technique for compressions
- 3:1 compressions:ventilations
- Target compression rate > 100 bpm
- In newborns > 35weeks gestation, resuscitation may begin with room air.
- In newborns < 35weeks gestation, resuscitation should begin with supplemental oxygen.
- NRP Guidelines recommend targeted SpO2 goals in first 10 minutes of life (measured on Right Arm):
- 1 minute: 60-65%
- 3 minutes: 60-75%
- 5 minutes: 80-85%
- 10 minutes: 85-95%
Protocol 311: Post-Cardiac Arrest with ROSC
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Return of Spontaneous Circulation (detectable pulse, measurable blood pressure) after cardiac arrest
- Increase in EtCO2 on capnography after return of pulse and blood pressure
Contraindications:
- Unable to maintain a pulse
- Unable to obtain a blood pressure
Procedure/Approach:
- Obtain pulse and blood pressure
- Oxygenate/ventilate as needed
- AEMT/Paramedic: Obtain 12 Lead EKG as soon as possible
- If STEMI, initiate CARDIAC ALERT Protocol and rapid transport
- Assess for shock
- 20ml/kg fluid bolus x 2 if needed
- Paramedic: contact Medical Control to consider vasopressor infusion
- Obtain IV/IO access if not already obtained
- Targeted ventilation
- Target EtCO2 of 30-35mmHg
- Secure Advanced Airway if not already performed
- Maintain AED/Monitor for recurring dysrhythmias
- If transport time permits, may consider Targeted Temperature Management
- Cold packs to junctional vessels
- Target to 91.4 – 96.0 degrees F
Considerations:
- Waveform Capnography is an excellent tool to evaluate both return of circulation and the effects of resuscitation and should be used to monitor both airway patency and the degree of metabolism post-ROSC.
- It is common to see ‘reperfusion arrhythmias’ after ROSC. If a pulse and BP remain detectable, interventions are not recommended for short interval arrhythmias (eg short burst of VTach, PVCs, etc). If a persistent dysrhythmia presents and results in change of pulse and BP, then intervene as per ACLS guidelines and these protocols.
Protocol 312: Unstable Tachycardia
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Tachycardia > 150 in adults with signs of shock or altered mental status
Contraindications:
- Heart rate below 150 in adults
- Age < 12= contact medical control
Procedure/Approach:
- Support ABCs
- Supplemental Oxygen
- AEMT/Paramedic: Identify 3 lead rhythm, perform 12 Lead EKG
- Identify QRS Width
- > 0.12 and REGULAR, Usually Ventricular Tachycardia
- < 0.12 OR IRREGULAR, Usually Supraventricular Tachycardia with or without an aberrancy, or Atrial Arrhythmia
- Paramedic: if patient in shock, prepare for immediate synchronized cardioversion
- Sedation with benzodiazepine if patient condition and time permits
- After cardioversion, repeat 12 Lead EKG
- If successful, monitor vitals, initiate transport
- If unsuccessful, may consider the following interventions based off of repeat 12 Lead interpretation:
- SVT- adenocard, vagal maneuvers
- Atrial arrhythmia- no medications, cardiovert or transport
- V Tach- Amiodarone, repeat cardioversion
- Torsades de Pointes- Magnesium Sulfate
- Contact Medical Control
- Identify QRS Width
Considerations:
- Pediatric patients under the age of 12 rarely require cardioversion. Contact medical control for their assistance in these rare circumstances.
- In general, if they do not convert after several attempts, initiate rapid transport and notify medical control.
Protocol 313: Unstable Bradycardia
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Any bradycardia resulting in altered mental status, cyanosis or hypotension
- Any bradyarrhythmia associated with chest pain
- Any heart block rhythm with associated altered mental status or hypotension
- Heart Rate < 60 with symptoms of syncope, chest pain or signs of shock
Contraindications:
- Arrhythmias associated with any trauma
- Pulseless electrical activity (refer to Medical Cardiac Arrest Protocol)
Procedure/Approach
- Assess ABCs
- Provide supplemental oxygen
- Obtain 12 Lead EKG
- Initiate large bore IV or IO
- Pediatric patients (< age 12)
a. If heart rate < 60bpm with poor perfusion, initiate CPR
b. Paramedic Only:
i. Use epinephrine as first line therapy for pediatric bradycardia
ii. Contact Medical Control for considerations for atropine or pacing
6. Paramedic Only:
a. Consider atropine unless there is a 3rd degree block or ventricular escape rhythm
b. Pre-medicate with benzodiazepine if time permits
c. Transcutaneous pacing
d. If pacing fails to capture, contact Medical Control for consideration of vasopressor infusion
7. Initiate Rapid Transport, and early notification to ER
Considerations:
- Consider HR < 60 in any ill child a critical finding, regardless of their age and level of consciousness.
- For any symptomatic bradycardia, consider possible contributing factors including the “5Hs and 5Ts” from PALS and ACLS protocols
- Evaluate the scene for any possible drug overdose, intentional or accidental (beta blockers or calcium channel blockers)
- ALWAYS perform a 12 Lead EKG. Often symptomatic bradycardia is a sign of an acute MI or acute electrolyte problem, such as hyperkalemia, which will present on 12 Lead.
Protocol 314: Chest Pain
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Chief complaint of chest pain
- Patients fitting a pattern of “Silent MI”: diabetic, female, elderly, or severe hypertension
Contraindications:
- No absolute contraindications
- Relative contraindications: age < 12 rarely demonstrate acute coronary syndromes
Procedure/Approach:
- Assess ABCs
- Titrate oxygen to SpO2 > 90%
- Administer aspirin 325mg
- AEMT/Paramedic:
a. Obtain 12 Lead EKG
i. IF STEMI à activate Cardiac Alert Protocol
ii. consider opioid for chest pain
b. Establish large bore IV
c. Consider repeat 12 Lead EKG at regular intervals
d. Consider additional views (right side, posterior side)
e. Fluid bolus for hypotension
f. Consider defibrillation pad placement for hypotension
5. Nitroglycerin SL for suspected cardiac chest pain ONLY IF:
i. No right sided STEMI on EKG
ii. No hypotension
iii. No use of erectile dysfunction medications
6. Consider Causes:
a. Myocardial Infarction → Aspirin, Cardiac Alert Protocol
b. Pulmonary Embolism → rapid transport
c. Thoracic Aortic Dissection → rapid transport
d. Tension Pneumothorax → Needle Decompression
e. Cardiac Tamponade → fluid bolus for hypotension, rapid transport
f. Myocarditis/Pericarditis → check temperature, IV fluids, transport
g. Congestive Heart Failure → CHF Protocol
Considerations:
- High flow oxygen has not been shown to improve outcomes. Titrate with nasal cannula unless high flow is required.
- Morphine is associated with worse survival rate. Utilize dilaudid or fentanyl for chest pain when using opioid medications.
- Aspirin is the only essential medication with suspected cardiac event, nitroglycerin is optional, especially in setting of lower blood pressures.
- Nitroglycerin should not be given as 3 automatic doses. Reassess blood pressure between each dose and hold further doses if any hypotensive change occurs.
- Repeat 12 Lead EKG when time permits and there is either a change in patient condition, complaint or vital signs. Myocardial infarctions commonly evolve and can show more obvious changes on subsequent EKGs.
Protocol 315: Cardiac Alert
Scope: Advanced EMT and Paramedic
Indications:
- 12 Lead EKG showing ST segment elevation at least 1mm in two or more contiguous leads
- Age 35 – 85 years old
Contraindications:
- Bundle Branch Block
- Outside of age range, consider contacting medical control for guidance
Procedure/Approach:
- Initiate Chest Pain protocol en route to hospital
- Transfer emergently, notifying ER as soon as possible, declaring CARDIAC ALERT
- Initiate TWO large bore peripheral IVs in forearm or above, sparing the wrists
- Transport with defibrillation pads in place
Considerations:
- In this region there are no cardiac catheter labs within 90 minutes of Sherman County, therefore the standard of care is to achieve rapid “door-to-drug” time of the administration of Tenecteplase (TNK) as thrombolytic therapy. The faster this is done, the greater the survival. This also facilitates more rapid planning for transport to a cardiac care facility.
- Aeromedical evacuation should NOT be requested to scene. TNK administered in local ER is preferable to air transport if a cath lab cannot be achieved within 90 minutes of 911 arrival on scene. In this region, a helicopter typically takes between 45 to 60 minutes under ideal circumstances to arrive, and then usually requires additional time on ground to refuel before transporting to Hays, KS or Parker, CO, the two closest cardiac cath labs. IV TNK at the local ER is preferable to delayed aeromedical evacuation under these circumstances.
Protocol 316: Ventricular Assist Devices
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Patients presenting with a Ventricular Assist Device and complaint of syncope, chest pain, trouble breathing or presenting with hypotension
Contraindications:
- Not applicable.
Procedure/Approach:
- Assess the Patient’s Hemodynamic status:
a. This requires BP determination with MANUAL BP cuff
b. Often requires pulse check at carotid or with doppler if patient has one with them
2. If patient is stable, address other medical problems and transport
3. If patient is unstable, auscultate chest for whirling/motor sounds
a. VAD is running- 250ml fluid bolus, rapid transport
b. VAD is NOT running:
i. Eval VAD for alarms, contact medical control for guidance
c. Initiate ACLS, including chest compressions and defibrillation if indicated
Considerations:
- https://www.mylvad.com/medical-professionals/resource-library/ems-field-guides is a useful website for details about LVADs.
- In general, any cardiac, respiratory or neurologic complaint associated with an LVAD requires ER evaluation.
Protocol 317: Pediatric BRUE
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Infant (less than 1 year of age) with episode frightening to the observer characterized by apnea, choking, gagging, color change or change in muscle tone
Contraindications:
- None.
Procedure/Approach:
- Evaluate ABC
- Provide oxygen and ventilation if needed
- Obtain detailed history of event and medical history
- All BRUE events require ER evaluation and should be transported
Considerations:
- Defer to Pediatric Respiratory Distress Protocol if any signs of continued respiratory distress.
Protocol 318: Anaphylaxis
Scope: EMT-Basic, Advanced EMT and Paramedic
Indications:
- Allergic reaction, anaphylaxis or angioedema
Contraindications:
- None.
Procedure/Approach:
- Evaluate airway
a. If evidence of airway obstruction due to swelling
i. Give IM epinephrine immediately
ii. Rapid Transport
iii. Paramedic Only: Contact Medical Control for consideration of Rapid Sequence Intubation
iv. Establish large bore IV / IO
2. Evaluate for signs of anaphylactic shock
a. Hypotension à consider fluid bolus by IV/IO
b. Give supplemental oxygen
c. Give IM epinephrine
d. Paramedic Only: if persistent hypotension, consider contacting medical control for epinephrine infusion (aka “dirty epi drip”)
e. Rapid Transport
3. Give diphenhydramine
4. Give methylprednisolone
5. Consider Albuterol if wheezing/bronchospasm is evident
Considerations:
- Evaluation of allergic/anaphylactic reactions include the following systems:
o Dermatologic: evaluate skin for hives, itching, dermatographia
o Airway: evaluate mouth/tongue for swelling, edema, stridor
o Respiratory: wheezing, bronchospasm
o Circulatory: hypotension, poor peripheral perfusion, chest tightness
o Gastrointestinal: nausea, vomiting, epigastric pain (from histamine release around the stomach)
o Neurologic: altered mentation (secondary to hypoxia or hypotension)
o ANY TIME an allergic reaction involves TWO OR MORE of these systems, it is considered ANAPHYLACTOID, and warrants consideration of epinephrine administration.
There are rare cases of a condition called familial angioedema, which results in sudden airway closure due to an autoimmune condition. This condition is life threatening and, importantly, DOES NOT respond to epinephrine/Benadryl/steroids, because it is not
caused by a release of histamine, but rather a bradykinin pathway of the immune system. If the patient or family mention this medical history, initiate RAPID TRANSPORT and early notification of MEDICAL CONTROL.